Introduction
What is a Concussion?
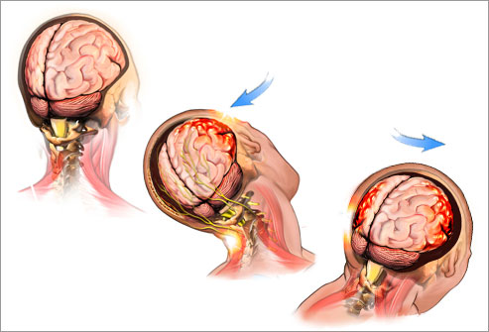
A concussion is caused by a jolt that shakes one’s brain back and forth inside your skull
Any hard hit to the head or body -- whether it's from a football tackle or a car accident -- can lead to a concussion.
Although a concussion is considered a mild brain injury, it can leave lasting damage if one dosen't rest long enough to let the brain fully heal afterward
|
Causes of Cognitive Deficits Related to TBI
- Brain injury
- Tinnitus-related psychological distress
- Insomnia
- Chronic headaches
- Depression
- PTSD
- Chronic Pain
Impact why problems with thinking, concentration and being able to think clearly
Many factor mimic, mask or exacerbate TBI or Post Concussive symptoms (PCS)
- Brain injury
- Vestibular injury
- Tinnitus-Related Psychological Distress
- Chronic Bodily Pain or Headaches
- Insomnia /Sleep Disturbance
- PTSD
- Anxiety/Stress/Somatic Preoccupation
- Life Stress
All cause symptoms similar to Post Concussive Symptoms
Typical Recovery Times from TBI
- Athletes: 1-28 days
- Civilians: 1 week to 6 months
- Service members coming out of combat: can be longer
Risk Factors for Long-Term Symptoms and Problems
Biological
- Genetic
- Injury severity
- Prior brain injury
Psychological
- Past mental health problems
- Resiliency
- Current traumatic stress and/or depression
Social/Environmental
- Life stress and problems with employment
- Litigation/Disability/Compensation issues
Post Concussive Symptoms
- Headaches
- Fatigue
- Noise Sensitivity
- Problems Concentrating
- Problems with Memory
- Sleep Disturbances
- Depression-has similar symptoms to PCS
Treatment Recommendations for Rehabilitation of Vets with TBI
- Focused, Evidence-Supported Treatment for Specific Symptoms & Problems
- Medications
- Physical Therapy
- Vestibular Rehabilitation
- Exercise
- Psychological treatment
Psychological Treatments for 1-2 year post Injury
- CBT especially if chronic depressed
- Self-management
- Behavioral Activation
- Stress Management
- Acceptance & Commitment Therapy
Exercise for individuals who have long term TBI Symptoms
Exercise as a component of a treatment Plan for patients with TBI
- Facilitates molecular markers of neuroplasticity & promotes neurogenesis healthy & injured brains
- Associated with changes in neurotransmitter systems associated with depression & anxiety
- Effective treatment or adjunctive treatment for mild forms of anxiety & depression
- Associated with reduced pain and disability in patients with chronic low back pain
- Regular long-term aerobic exercise reduces migraine frequency, severity & duration
|
Goal for Patients with Complex Comorbidities with mTBI to Improve Functioning
Reduce Sleep Disturbance
Lessen Stress & Anxiety Symptoms
Lessen Depressive Symptoms
Deconditioning from pattern of responses to Triggers
Reduction of HeadachesReduction of Bodily Pain
Treat what you can treat!
|
Let's Look at What has Happened to our Vets
CASE STUDY
Corporal (Cpl) Buchanan is a 22-year-old USMC CBRN Defense Specialist (5711) who was the gunner in a Military All-Terrain Vehicle when it struck a 40-lb Improvised Explosive Device. Cpl Buchanan lost consciousness for 5 seconds and experienced 15 seconds of post-traumatic amnesia He was diagnosed with a concussion
–Symptoms: 5/10 headache, confusion, dizziness and nausea
Cpl Buchanan was given 24 hours of mandatory recovery (rest) and acetaminophen for headache. He entered stage one (rest) for 24 additional hours, then advanced through the following stages of the progressive return to activity clinical recommendation:
- Stage two: Light routine activity
- Stage three: Light occupation-oriented activity
- Stage four: Moderate activity
- Stage five: Intensive activity
After 5 days, Cpl Buchanan presented as follows:
- All symptoms have resolved, except for an ongoing difficulty with sleep which he minimized and denied on the Neurobehavioral Symptom Inventory (NSI)
- Automated Neuropsychological Assessment Metrics scores returned to baseline
- Passed exertional testing
- Returned to unrestricted duty
Cpl Buchanan’s tour ended 4 months after his injury and he returned home
Upon his return home, the Cpl reported to his primary care manager (PCM) with the following complaints:
- 4 months of difficulty sleeping (2 hours or more to fall asleep and difficulty staying asleep)
- Using daily energy drinks to stay awake
- Difficulty remembering information
- Difficulty paying attention to conversations
- Increased irritability
The PCM completed a clinical sleep interview, physical examination and administered a self-report measure
Clinical Sleep Interview
- Difficulty falling asleep, daytime fatigue and nightmares
- No complaints of snoring or gasping for air during sleep
- Reports excessive daily caffeine intake (600-700 mg/day)
- No sleep-specific red flags
Physical Examination
- Body mass index (BMI) and blood pressure are within normal limits
Self-report Measure
- Insomnia Severity Index (ISI) reveals a score of 17
The PCM diagnosed Cpl Buchanan with chronic insomnia and instructed him in the following:
- Stimulus control
- Sleep hygiene
- Progressive muscle relaxation training
After 2 weeks of treatment and weekly PCM appointments, Cpl Buchanan reported only mild improvement
The PCM referred him for Cognitive Behavioral Therapy for Insomnia (CBT-I)
Cpl Buchanan reported only mild improvement after 4 weeks of full CBT-I
The PCM administered the Insomnia Severity Index (ISI) again, which revealed a score of 14 (three point improvement)
The PCM referred Cpl Buchanan to a sleep medicine specialist
- Further diagnostic workup confirmed chronic insomnia
- Recommended treatment included:
- Acupuncture
- Behavioral health evaluation and treatment
After 3 weeks, Cpl Buchanan reported the following improvements:
- Decreased daytime fatigue
- Significantly improved ability to fall asleep
- Decreased frequency of nightmares
- Improved ability to pay attention and remember information
- Decreased irritability
|
Vets who return with TBI or PTSD don't just have Mental Health issues but also physical injuries
- Orthopedic injuries: chronic pain due to joint and muscular-skeletal injuries in back, knees, shoulders, wrists
- Hearing problems: hearing loss, ringing in ears
- Respiratory illnesses: sand, dust
- Skin conditions: rashes, bacterial infections
- Major trauma injuries: gunshot wounds, shrapnel, traumatic brain injuries
|
What’s Keeping the New Veterans from Seeking Care?
Practical Concerns/Logistical Barrier
- I don’t know where to get help
- I don’t have adequate transportation
- It’s difficult to schedule an appointment
- It’s difficult getting time off work
- Costs too much money
- I don’t trust mental health professionals
(Hoge et al. 2004, NEJM; Ouimette et al., 2011)
Impact of Stigma in Seeking Help
Stigma (active duty)
- It would harm my career
- Members of my unit might have less confidence in me
- Unit leadership might treat me differently
- Leaders would blame me for the problem
Stigma (veterans & active duty)
- I would be seen as weak; I would see myself as weak
- It would be too embarrassing
- I don’t want other people to know about my problems
- I don’t like to get emotional about things
|
What is TBI?
- Effects of a typical IED in Afghanistan on Military ATV
- Weapon of choice by the enemy
- IEDs are a daily threat to all ground forces.
- If someone has been involved in a blast (within 100 meters) and has not been assessed there is a possibility of mTBI
- Majority of mTBI sustained by service members occur during daily life or military training, not during deployment and while deployed ie: playing sports
|
The Brain Is the Organ of Coping
Coping: “the person’s constantly changing cognitive and behavioral efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the person’s resources.” (Lazarus & Folkman, 1984)
Coping (whether adaptive or maladaptive) depends on intact higher cortical functioning
- Cognitive appraisal (thinking)
- Enacting a coping strategy (doing)
The performance limits of the brain, therefore, define the limits of adaptive coping
|
Reasons for comorbidities with TBI
The structure and functioning of the CNS set limits on capacities for coping and all other behavior
Mental disorders are the result of losses of integrity in the CNS rather than maladaptive coping choices
- PTSD
- Major depressive disorder
- Generalized anxiety disorder
- Psychotic disorders
To think and teach otherwise is to blame our patients for their own suffering
|
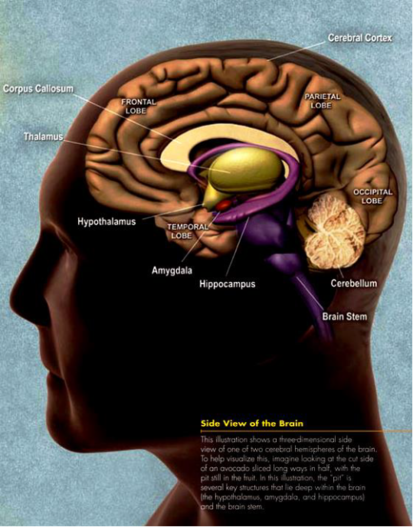
Regions of Cortex Involved in Self Regulation
Medial PFC
- Volitional control of emotion
Orbitofrontal PFC
Dorsolateral PFC
- Volitional control of attention
Insula
- Volitional control of arousal
Together, these regions of prefrontal and insular cortex make possible inhibition and control of emotions, thoughts, behaviors, and physiological arousal
|
Hippocampus:
Gray-Matter Partner to Prefrontal Cortex (PFC)
Functions
- Declarative memory: laying down and consolidation of recallable memory
- Inhibition (along with PFC)
- Fear extinction
- Spatial mapping (GPS)
- May also be crucial for constructing a coherent mental image, whether from current perception or memory
|
Amygdala:
Important Target for Control by PFC and Hippocampus
Functions
- Puts “emotional stamp” on memories
- Fear, anger, (etc.?)
- Threat detector
- Social recognition
- Fear conditioning
- Appetite conditioning?
|
Nucleus Accumbens:
Another Important Target for Control By PFC and Hippocampus
Functions
- Reward, pleasure
- Well-being
- Motivation
- Focus, attention
- Goal-directed behavior
- Addiction, craving
|
A Few Molecular Modulators of Stress
- Corticotropin-releasing factor (CRF)
- Cortisol
- Brain-derived neurotrophic factor (BDNF) and other neurotropins
- Glutamate (Glu) acting at N-methyl-d-aspartate (NMDA) receptors
Corticotropine-releasing factor (CRF), Cortisol, and Brain-derived neurotrophic factor (BDNF)
CRF is the master stress modulator (“on” switch for stress)
CRF is both:
- A hormone released in the hypothalamus triggering release of corticosteroids like cortisol from adrenal cortex
- A neurotransmitter used by a diffuse network of neurons in the brain
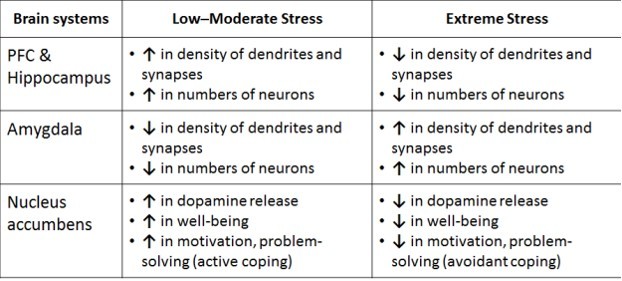
Both CRF and cortisol have biphasic activity in the brain:
- At low to moderate levels, they improve performance, learning, and well-being
- At high or sustained levels, they degrade performance, learning, and well-being
Cortisol interacts with BDNF to stimulate growth of new dendrites, synapses, and entire neurons, but in different brain systems depending on stress level
|
COMORBIDITIES OF TBI
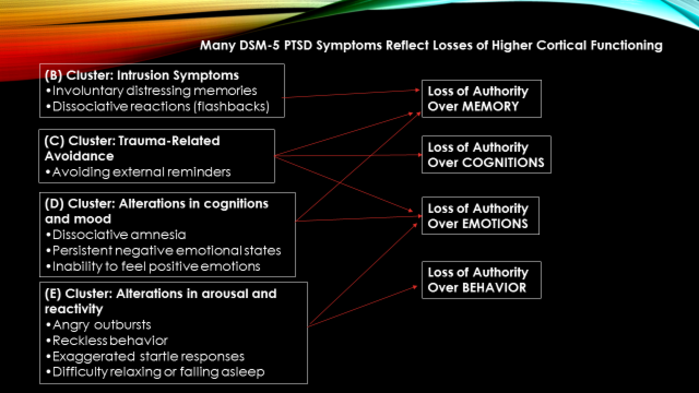
PTSD Criteria
Traumatic experience(s)
- Intrusion
- Avoidance
- Alterations in cognition & mood
- Alterations in arousal
- Functional interference
Checklist for PTSD
Re-experience the event over and over again
- You can’t put it out of your mind no matter how hard you try
- You have repeated nightmares about the event
- You have vivid memories, almost like it was happening all over again
- You have a strong reaction when you encounter reminders, such as a car backfiring
Avoid people, places, or feelings that remind you of the event
- You work hard at putting it out of your mind
- You feel numb and detached so you don’t have to feel anything
- You avoid people or places that remind you of the event
Feel “keyed up” or on-edge all the time
- You may startle easily
- You may be irritable or angry all the time for no apparent reason
- You are always looking around, hyper-vigilant of your surroundings
- You may have trouble relaxing or getting to sleep
|
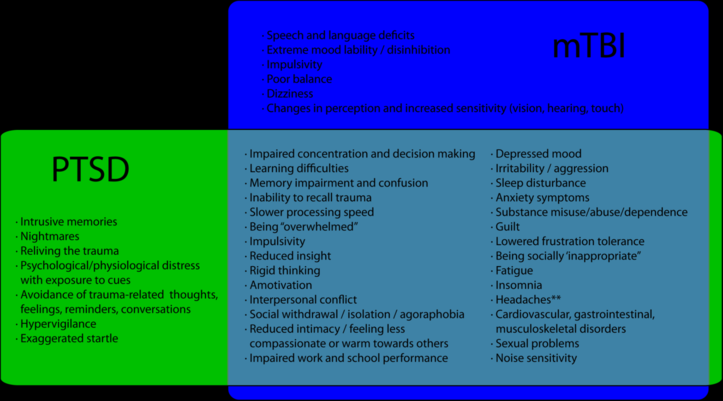
Traumatic Stress or Post Concussive Symptoms
Overlap of PTSD and TBI Symptoms
- Concentration, attention, sleep etc
- Examine onset: target trauma & TBI may not be the same event
- Look at developmental history prior to deployment to see if there is a change in function
- Identify level of severity of symptoms
- If comorbid with PTSD, treat the PTSD and see what symptoms remain
|
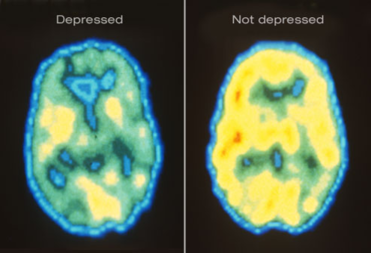
Symptoms of Depression
Cognitive Problems
- Memory
- Concentration, attention and focusing
- Learning and understanding new things
- Processing & understanding information including following complicated directions
- Language problems
- Problem-solving, organization, decision-making
- Impulse control
- Slowed or cloudy thinking
- Negative beliefs about self, world & future
Affective/Behavioral Problems
- Frustration or irritability
- Depression/sad
- Anxiety
- Reduced tolerance for stress
- Sleep problems
- Numbing out or flipping out
- Inflexibility
- Feeling less compassionate or warm towards others
- Feeling guilty
- Feeling helpless/hopeless
- Denial of problems
- Social appropriateness
Somatic Complaints
- Headache
- Fatigue
- Poor balance
- Dizziness
- Changes in vision, hearing, or touch
- Sexual problems
|
Sleep disorders are common after concussion
Service Persons with physical, cognitive or behavioral/emotional symptoms following concussion should be screened
- Insomnia is the most common sleep disturbance following concussion
- Primary care diagnosis and management is facilitated by a focused sleep assessment
- Non-pharmacological measures are the foundation for care, to include stimulus control and sleep hygiene
Referral to a sleep medicine specialist may be necessary or likely
- Especially for chronic insomnia (after initial management
- Sleep disturbances can significantly exacerbate or impact other concussion symptom
Sleep Assessment Form (below)
|
Cognitive Behavioral Therapy for Insomnia (CBT-I) is most effective treatment for insomnia
|
Pain
Chronic Pain is a common issue of OEF and OIF Returning Veterans
It can hide or exacerbate TBI or PTSD Symptoms
Pain needs to be treated
|
VA/DoD Expert Consensus Guidelines
1.Assessment: What are the best approaches to assess, PTSD, history of mTBI and pain in Veterans presenting for treatment? Use diagnostic tools to screen for all three. Determine comorbidities and if the symptoms are current or historical. Rule out possibility of depression and substance abuse
2.Treatment Planning: What are the challenges of treatment planning with a Veteran comorbid PTSD, pain & history of mTBI? Make sure patient has an understanding of what treatments will be used for which symptoms
3.Treatment: What do practice guidelines tell us about the most effective PTSD, pain & a history of mTBI treatment strategies? Use guideline for all 3 specific conditions. Deliver a consistent message which is encouraging for recovery.
Evidence Based Practices for PTSD, TBI and Pain
PTSD: Prolonged Exposure or Cognitive Processing Therapy
TBI: Rehabilitation interventions
Pain: Rehabilitation interventions
- Use psychoeducation to help them to recognize that pain has a role as trigger for PTSD & increased anxiety
- After treat PTSD, consider CBT for Chronic Pain
|
Assessments of TBI Comorbidities
Overall Symptom Assessment
- Neurobehavioral Symptom Inventory (NSI)
TBI
- DVBIC 3 Question TBI Screening Tool
- Military Acute Concussion Evaluation (MACE)
PTSD
- PCL (PTSD Checklist)
- CAPS
- Combat Exposure Scale (CES)
Sleep Disorder
- Berlin Questionnaire
- Insomnia Severity Index
- Morningness-Eveningness Questionnaire
- STOP-BANG Questionnaire
- Epworth Sleepiness Scale
PAIN
- Initial Pain Assessment
- Initial Pain Assessment Tool
- Patient Comfort Assessment Guide
- Visual Analog Scale
- Wong-Baker Faces Pain Rating Scale
Complete listing of Assessments for Comorbidities of TBI are located on coping.us at:
|
APPS For TBI related Comorbidities
MTBI
PTSD
- PE Coach
- PTSD Coach
- CPT Coach
Sleep
Addictions
Depression & Anxiety
- T2Mood Tracker
- Tactical Breather
- Breathe2Relax
- LifeArmor
- Goal Setting
Suicide Prevention
- Moving Forward
- Safe Helpline
- ASK
|
Treatment Manuals For TBI related Comorbidities
PTSD:
Foa, E.B., Hembree, E.A. & Rothbaum, B.O. (2007). Prolonged Exposure Therapy for PTSD Emotional Processing of Traumatic Experiences Therapist Guide. NY: Oxford University Press.
Resick, P.A., Monson, C.M. & Chard, K. M. (2008). Cognitive Processing Therapy Veteran/Military Version: Therapist Manual. Washington, D.C.: Department of Veterans Affairs.
Pain Related:
Otis, J.D. (2007). Managing Chronic Pain A Cognitive-Behavioral Therapy Approach. NY: Oxford University Press.
Rollnick, S., Miller, W.R. & Butler, C. C. (2008). Motivational Interviewing in Health Care. Helping Patients Change Behaviors. NY: Guilford Press.
Sleep Related:
DCoE (2014) Management of Sleep Disturbances Following Concussion/Mild Traumatic Brain Injury: Guidance for Primary Care Management in Deployed and Non-Deployed Settings: Washington, DC: Author
Edinger, J.D. & Carney, C.E. (2008). Overcoming Insomnia A Cognitive-Behavioral Therapy Approach. NY: Oxford University Press
Substance Use Disorders:
Daley, D.C. & Marlatt, G. A. (2006) Overcoming Your Alcohol or Drug Problem: Effective Recovery Strategies. NY: Oxford University Press
Epstein, E.F. & McCrady, B.S. (2009) A Cognitive-Behavioral Treatment Program for Overcoming Alcohol Problems. NY: Oxford University Press
|
Top 10 Tips to Promote Successful Coping with Comorbidities of TBI
1. Stay physically active: Exercise daily. Avoid impairment and disability due to becoming physically inactive (“If you don’t use it, you will lose it”)
2. Stay mentally active: Learn something new every day. Exercise your brain with daily “brain jogging,” such as reading books, newspapers, and magazines. Again: “Use it or lose it.”
3. Stay connected to other people: Treasure and nurture the relationships you have with your spouse/partner, your family, friends, and neighbors. Reach out to others—including younger people. Stay involved in your community.
4. Don’t sweat the small stuff: Don’t worry too much. Be flexible and go with the flow. Don’t lose sight of what really matters in life.
5. Set yourself goals and take control: It is important to have meaningful goals in life and to take control in achieving them. Being in control of things gives us a sense of mastery and usually leads to positive accomplishments.
6. Create positive feelings for yourself: Experiencing positive feelings is good for our body, our mental health, and for how we relate to the world around us. Feeling good about our own age is part of this.
7. Minimize life stress: Many illnesses are related to life stress, especially chronic life stress. Stress has a tendency to “get under our skin,” if we notice it or not. Try to minimize stress and learn to unwind and “smell the roses.”
8. Adopt healthy habits: Maintain optimal body weight. Eat healthy food in small portions. Drink alcohol in moderation. Quit smoking. Floss your teeth. Adopt good sleeping habits.
9. Have regular medical check-ups: Take advantage of health screenings and engage in preventive health behavior. Many symptoms and illnesses can be successfully managed if you take charge and if you partner with your health care providers.
10. It is never too late to start working on Tips 1 through 9: It is never too late to make changes.
|
Goal for Patients with Complex Comorbidities to Improve Functioning
- Reduce Sleep Disturbance
- Lessen Stress & Anxiety Symptoms
- Lessen Depressive Symptoms
- Deconditioning from pattern of responses to Triggers
- Reduction of Headaches
- Reduction of Bodily Pain
Treat what you can treat!
|
|