Adverse Childhood Experiences
(ACE) Factors Assessment
|
|
Clinician Treatment Tools
|
|
|
COPING.US Training Programs: ACE Factors Presentation
Use of Adverse Childhood Experiences (ACE Factors) in Clinical Assessment
CEU’s: 3 hours based on request (CE Broker Tracking #: 20-615466)
Resource for Course on Coping.us:
http://www.coping.us/cliniciantreatmenttools/acefactors.html
and
http://www.coping.us/layingthefoundation.html
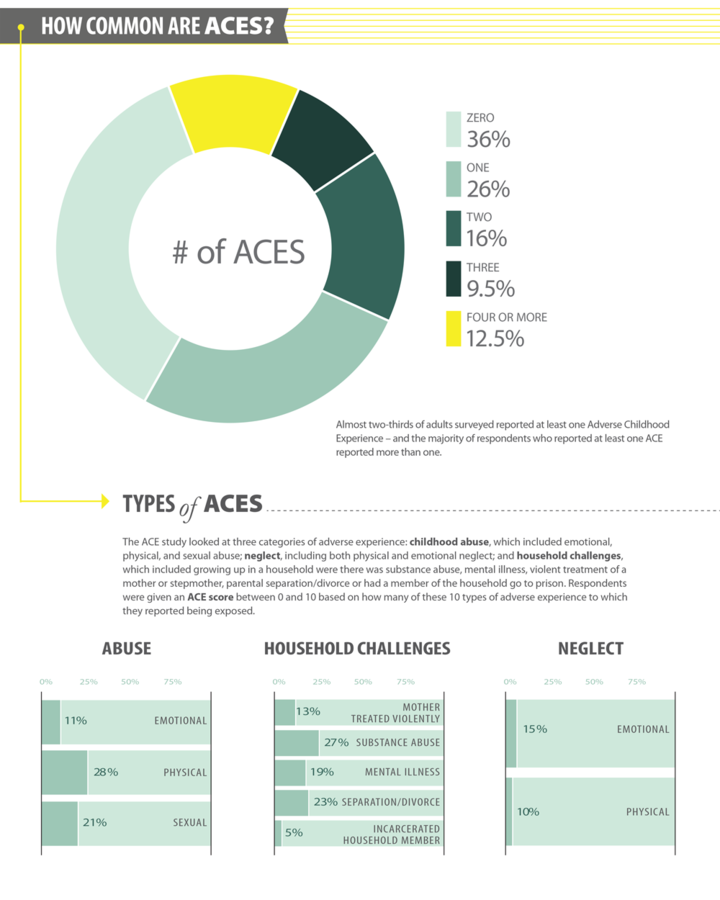
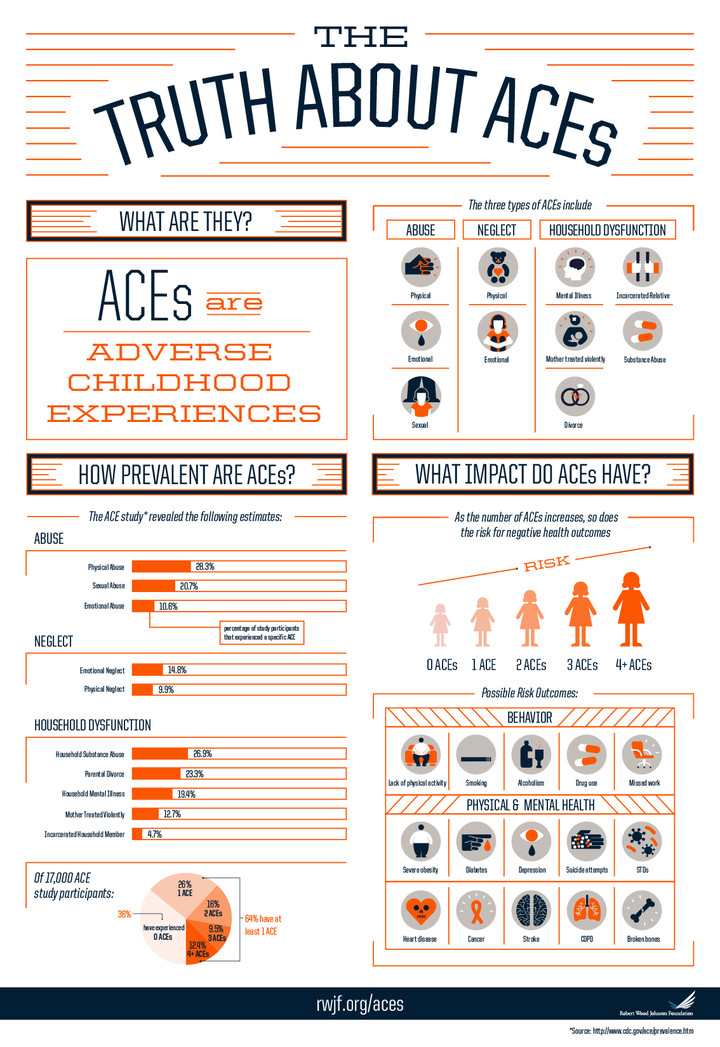
Program Description: This program is focused on the need to address ACE Factors in the initial assessment with clients when doing a psychosocial history. It is important that Mental Health Professionals understand the impact of these ACE Factors which are: Emotional Abuse, Physical Abuse, Sexual Abuse, Emotional Neglect, Physical Neglect, Mother who was treated violently, Household Substance Abuse, Household Mental Illness, Parental Separation or Divorce and Incarcerated Household Member. Since 1995 when the CDC did research on 17,000 patients, it was shown that adults who suffered from one or more of the ACE Factors before they reached 18 years of age were more likely to: I. have reduced physical activity, 2. Smoke, 3. Excessive Alcohol Use, 4. Drug Use and 5. Missed Work or had chronic health conditions 1. Obesity, 2. Diabetes, 3. Depression, 4. Suicide Attempts, 5. Sexually Transmitted Diseases, 6. Heart Disease, 7. Cancer, 8. Stroke, 9. COPD or 10. Broken Bones. For this reason, it is imperative that this information be discovered and included both In the Initial Clinical Assessment but also incorporated into the Initial Clinical Treatment Plan. This issue is so pressing the DSM-5 utilized the ACE Factors in setting up their Other Conditions That May Be a Focus of Clinical Attention in the diagnostic process. Included in this workshop will be an overview of personality characteristics which are common of survivors of families which are classified as being dysfunctional.
Learning Objectives:
1. To learn about the impact ACE Factors in America today with an exploration of what are the underlying sociological, psychological and physiological issues which are at the root of the impact of the ACE Factors.
2. To learn about how to assess for ACE Factors as well as assess for Protective Factors in clients' histories so as to get a more complete grasp of the lifestyles which have contributed to current mental health and/or physical health functioning.
3. To learn how to use the DSM-5 diagnosing terminology to accurately identify the "non-mental health disorder" conditions which could undermine treatment for the principal diagnosis of the clients and to recognize that these factors stay with adults for their whole lives.
4. To learn about the movement in American to intervene with youth at an early age with Trauma Focused Cognitive Behavioral Therapy to help youth who have suffered ACE Factors to gain resilience and ability to move forward with their lives in a productive way.
|
Use the ACE Factors in all of Your Initial Clinical Assessment
You can use the following survey to help identify the presence of ACE Factors in your client's life.
|
Directions: Here are some questions about events that happened during your childhood. This information will allow you to better understand problems that may occur early in life, and may help others in the future. All questions refer to the time before you were 18 years of age.
Response Options
|
Questions 1-4
1=Yes
2=No
7=DK/NS
9=Refused
|
Question 5
1=Yes
2=No
8=Parents not married
7=DK/NS
9=Refused
|
Questions 6-11
1=Never
2=Once
3=More than once
7=DK/NS
9=Refused
|
Now, looking back before you were 18 years of age:
____1. Did you live with anyone who was depressed, mentally ill, or suicidal?
____2. Did you live with anyone who was a problem drinker or alcoholic?
____3. Did you live with anyone who used illegal street drugs or who abused prescription medications?
____4. Did you live with anyone who served time or was sentenced to serve time in a prison, jail, or other correctional facility?
____5. Were your parents separated or divorced?
____6. How often did your parents or adults in your home ever slap, hit, kick, punch or beat each other up?
____7. Before age 18, how often did a parent or adult in your home ever hit, beat, kick, or physically hurt you in any way? Do not include spanking.
____8. How often did a parent or adult in your home ever swear at you, insult you, or put you down?
____9. How often did anyone at least 5 years older than you or an adult, ever touch you sexually?
____10. How often did anyone at least 5 years older than you or an adult, try to make you touch sexually?
____11. How often did anyone at least 5 years older than you or an adult, force you to have sex?
*These questions come from the CDC’s Behavioral Risk Factor Surveillance System Survey (BRFSS) Adverse Childhood Experience (ACE). Retrieved at: http://www.cdc.gov/violenceprevention/acestudy/pdf/brfss_adverse_module.pdf
|
What are ACE Factors
According to the CDC, Childhood experiences, both positive and negative, have a tremendous impact on future violence victimization and perpetration, and lifelong health and opportunity. As such, early experiences are an important public health issue. Much of the foundational research in this area has been referred to as Adverse Childhood Experiences (ACEs). Adverse Childhood Experiences have been linked to risky health behaviors, chronic health conditions, low life potential, and early death. As the number of ACEs increases, so does the risk for these outcomes.
The CDC-Kaiser Permanente Adverse Childhood Experiences (ACE) Study is one of the largest investigations of childhood abuse and neglect and later-life health and well-being. The original ACE Study was conducted at Kaiser Permanente from 1995 to 1997 with two waves of data collection. Over 17,000 Health Maintenance Organization members from Southern California receiving physical exams completed confidential surveys regarding their childhood experiences and current health status and behaviors. The CDC continues ongoing surveillance of ACEs by assessing the medical status of the study participants via periodic updates of morbidity and mortality data. Their study found a strong graded relationship between the breadth of exposure to abuse or household dysfunction during childhood and multiple risk factors for several of the leading causes of death in adults (Feliitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss, & Marks, 1998).
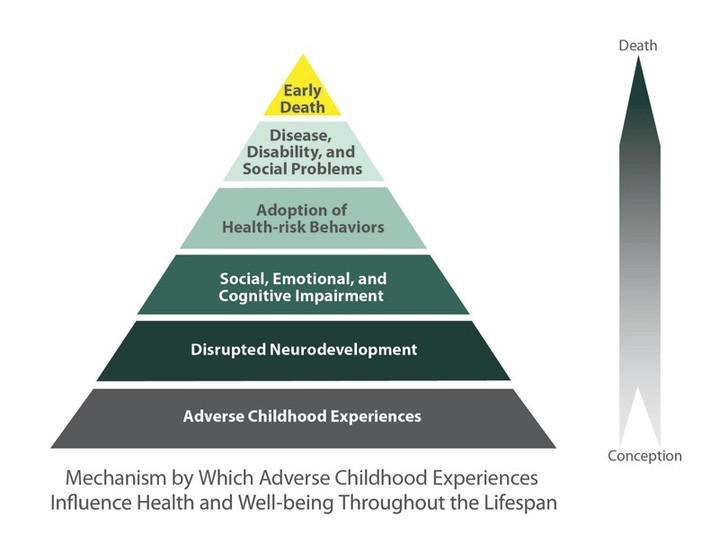
The following Chart demonstrates how the ACE factors initially impact early neurodevelopment and then Social, Emotional and Cognitive Development which impacts the development of Negative and Positive Core Beliefs for Individuals, which leads to Health-risky Behaviors and eventually Disease, Disability and/or Social Problems and in many cases early death
|
The ACE Pyramid represents the conceptual framework for the ACE Study. The ACE Study has uncovered how ACEs are strongly related to development of risk factors for disease, and well-being throughout the course of life.
ACE Factors affect behaviors of those who have one or more ACE factors in the following: 1. Lack of physical activity, 2. Smoking, 3. Alcoholism, 4. Drug use and 5. Missed work.
ACE factors affect the physical and mental health of those who have one or more ACE factors in the following: 1. Severe Obesity, 2. Diabetes, 3. Depression, 4. Suicide Attemps, 5. Sexually Transmitted Diseases (STDs), 6. Heart Disease, 7. Cancer, 8. Stroke, 9. COPD and 10. Broken Bones
Given the impact of ACE factors on both physical and mental health, it is important in working with clients that we identify if have have indeed experienced any Adverse Childhood Experiences which have influenced their Core Beliefs which need to be changed so as to improve both their physical and mental health.
You can get more on the ACE Factors at: http://www.cdc.gov/violenceprevention/acestudy/about_ace.html
|
Keep the ACE Criteria into Consideration when Doing an Initial Assessment
The Center for Disease Control has done studies on the impact of Adverse Childhood Experiences on the health of individuals. The ACE study has found that these adverse experiences are major risk factors leading to mental illness and poor quality of life. These adverse childhood experiences must be related to when doing a initial assessment of clients.
Download Questionnaires on the ACE called the Behavioral Risk Factor Surveillance System Survey (BRFSS) Adverse Childhood Experience (ACE) Module
|
|
For more background on ACE Factors
Watch a TED Talk by Dr Nadine Burke Harris on How childhood trauma affects health across a lifetime at: https://www.youtube.com/watch?v=95ovIJ3dsNk
To learn more about Trauma Focused Therapy Cognitive Behavioral Therapy which is mentioned in the ACE materials go to: http://tfcbt.musc.edu/. On this site you are able to take an online course in TFCBT as well.
|
ACE Factors Related References (can download PDF's by clicking on Title)
Reporting on ACE Factors in Your Clinical Assessment
Use the following format to report ACE factors in your reports:
ACE (Adverse Childhood Experiences)
Abuse
1. Emotional Abuse
2. Physical Abuse
3. Sexual Abuse
Neglect
4. Emotional Neglect
5. Physical Neglect
Household Dysfunction
6. Mother was treated violently
7. Household substance abuse
8. Household mental illness
9. Parental separation or divorce
10. Incarcerated household member
|
|
In Determining Diagnosis of a Client's Conditon it is important to:
- Rule in or rule out any Adverse Childhood Experiences (ACE Factors) by doing a thorough Psychosocial History Screening
- Identify the Diagnosis (es) as DSM-5 Principal and/or Provisional Diagnoses
- Identify Other Condition That May be a Focus of Clinical Attention (in DSM-5 at pp. 715-727) which are related to the ACE Factors which could interfere in the treatment of the client if not addressed as potential Trauma and/or Stressor related condition(s)
Relevant ACE (Adverse Childhood Experiences) Paired with
DSM-5’s Other Conditions That May Be a Focus of Clinical Attention
|
|
Abuse
1. Emotional Abuse
For Adults:
Z62.811 Personal history (past history) of psychological abuse in childhood
Z69.010 Encounter for mental health services for victim of child psychological abuse by parent
Z69.020 Encounter for mental health services for victim of nonparental child psychological abuse
Z91.49 Other Personal History of Psychological Trauma
For Children
T74-32XA Child Psychological Abuse Confirmed Initial Contact
T74-32XD Child Psychological Abuse Confirmed Subsequent Contact
T76-32XA Child Psychological Abuse Suspected Initial Contact
T76-32XD Child Psychological Abuse Suspected Subsequent Contact
Z69.010 Encounter for mental health services for victim of child psychological abuse by parent
Z69.020 Encounter for mental health services for victim of nonparental child psychological abuse
Z91.49 Other Personal History of Psychological Trauma
2. Physical Abuse
For Adults:
Z69.810 Personal history (past history) of physical abuse in childhood
Z69.010 Encounter for mental health services for victim of child abuse by parent
Z69.020 Encounter for mental health services for victim of nonparental child abuse
For Children:
T74-12XA Child Physical Abuse Confirmed Initial Contact
T74-12XD Child Physical Abuse Confirmed Subsequent Contact
T76-12XA Child Physical Abuse Suspected Initial Contact
T76-12XD Child Physical Abuse Suspected Subsequent Contact
Z69.010 Encounter for mental health services for victim of child abuse by parent
Z69.020 Encounter for mental health services for victim of nonparental child abuse
3. Sexual Abuse
For Adults:
Z69.810 Personal history (past history) of sexual abuse in childhood
Z69.010 Encounter for mental health services for victim of child sexual abuse by parent
Z69.020 Encounter for mental health services for victim of nonparental child sexual abuse
For Children:
T74-22XA Child Sexual Abuse Confirmed Initial Contact
T74-22XD Child Sexual Abuse Confirmed Subsequent Contact
T76-22XA Child Sexual Abuse Suspected Initial Contact
T76-22XD Child Sexual Abuse Suspected Subsequent Contact
Z69.010 Encounter for mental health services for victim of child sexual abuse by parent
Z69.020 Encounter for mental health services for victim of nonparental child sexual abuse
Z69.810 Personal history (past history) of sexual abuse in childhood
Neglect
4. Emotional Neglect
For Adults:
Z62.820 Parent-child relational problem
Z62.891 Sibling relational problem
Z62.29 Upbringing away from parents
Z62.898 as Child affected by parental relationship distress
Z63.0 Relationship distress with spouse or intimate partner
Z63.5 Disruption of family by separation or divorce
Z63.8 High expressed emotion level within family
Z62.896 Uncomplicated bereavement
For Children:
Z62.820 Parent-child relational problem
Z62.891 Sibling relational problem
Z62.29 Upbringing away from parents
Z62.898 Child affected by parental relationship distress
Z63.5 Disruption of family by separation or divorce
Z63.8 High expressed emotion level within family
Z62.896 Uncomplicated bereavement
64.0 Problems related to Unwanted Pregnancy
5. Physical Neglect
For Adults
Z69.812 Personal history (past history) of neglect in childhood
Z69.010 Encounter for mental health services for victim of child neglect by parent
Z69.020 Encounter for mental health services for victim of nonparental child neglect
For Children:
T74-02XA Child Neglect Confirmed Initial Contact
T74-02XD Child Neglect Confirmed Subsequent Contact
T76-02XA Child Neglect Suspected Initial Contact
T76-02XD Child Neglect Suspected Subsequent Contact
Z69.010 Encounter for mental health services for victim of child neglect by parent
Z69.020 Encounter for mental health services for victim of nonparental child neglect
Z69.812 Personal history (past history) of neglect in childhood
Z64.0 Problems related to Unwanted Pregnancy
Household Dysfunction
6. Mother was treated violently
Z62.898 Child affected by parental relationship distress
Z63.8 High expressed emotion level within family
Z65.9 Unspecified Problems Related to Unspecified Psychosocial Circumstances
Z75.4 Unavailability or Inaccessibility of Other Helping Agencies
Z75.3 Unavailability or Inaccessibility of Health Care Facilities
Z60.9 Unspecified Problem Related to Social Environment
Z60.9 Unspecified Problem Related to Social Environment
Z59.1 Inadequate Housing
Z59.4 Lack of Adequate Food or Safe Drinking Water
Z59.5 Extreme Poverty
Z59.6 Low Income
Z59.7 Insufficient Social Insurance or Welfare Support
Z59.9 Unspecified Housing or Economic Problems
7. Household substance abuse
Z63.8 High expressed emotion level within family
Z65.9 Unspecified Problems Related to Unspecified Psychosocial Circumstances
Z91.89 Other Personal Risk Factors
Z60.9 Unspecified Problem Related to Social Environment
Z60.9 Unspecified Problem Related to Social Environment
Z59.1 Inadequate Housing
Z59.4 Lack of Adequate Food or Safe Drinking Water
Z59.5 Extreme Poverty
Z59.6 Low Income
Z59.7 Insufficient Social Insurance or Welfare Support
Z75.3 Unavailability or Inaccessibility of Health Care Facilities
Z75.4 Unavailability or Inaccessibility of Other Helping Agencies
Z59.9 Unspecified Housing or Economic Problems
8. Household mental illness
Z63.8 High expressed emotion level within family
Z65.9 Unspecified Problems Related to Unspecified Psychosocial Circumstances
Z91.89 Other Personal Risk Factors
Z75.4 Unavailability or Inaccessibility of Other Helping Agencies
Z75.3 Unavailability or Inaccessibility of Health Care Facilities
Z60.9 Unspecified Problem Related to Social Environment
Z60.9 Unspecified Problem Related to Social Environment
Z59.1 Inadequate Housing
Z59.4 Lack of Adequate Food or Safe Drinking Water
Z59.5 Extreme Poverty
Z59.6 Low Income
Z59.7 Insufficient Social Insurance or Welfare Support
Z59.9 Unspecified Housing or Economic Problems
9. Parental separation or divorce
Z62.29 Upbringing away from parents
Z91.89 Other Personal Risk Factors
Z63.8 High expressed emotion level within family
Z75.4 Unavailability or Inaccessibility of Other Helping Agencies
Z75.3 Unavailability or Inaccessibility of Health Care Facilities
Z65.9 Unspecified Problems Related to Unspecified Psychosocial Circumstances
Z60.9 Unspecified Problem Related to Social Environment
Z59.1 Inadequate Housing
Z59.4 Lack of Adequate Food or Safe Drinking Water
Z59.5 Extreme Poverty
Z59.6 Low Income
Z59.7 Insufficient Social Insurance or Welfare Support
Z59.9 Unspecified Housing or Economic Problems
10. Incarcerated household member
Z62.29 Upbringing away from parents
Z91.89 Other Personal Risk Factors
Z63.8 High expressed emotion level within family
Z75.4 Unavailability or Inaccessibility of Other Helping Agencies
Z75.3 Unavailability or Inaccessibility of Health Care Facilities
Z65.1 Imprisonment or Other Incarceration
Z65.2 Problems Related to Release from Prison
Z65.3 Problems Related to Other Legal Circumstance
V62.9 Z65.9 Unspecified Problems Related to Unspecified Psychosocial Circumstances
Z60.9 Unspecified Problem Related to Social Environment
Z60.9 Unspecified Problem Related to Social Environment
Z59.1 Inadequate Housing
Z59.4 Lack of Adequate Food or Safe Drinking Water
Z59.5 Extreme Poverty
Z59.6 Low Income
Z59.7 Insufficient Social Insurance or Welfare Support
Z59.9 Unspecified Housing or Economic Problems
|
|
Expanded Interview Protocols to Use with Clients to assess their Family & Personal Health History
Knowing that ACE Factors have a major impact on both the physical and mental health of clients it is important to gain more information about the Health History of the specific client's familiy if we are working in an Integrated Medicine Setting or working at encouraging Wellness Programming for clients in your program
You can download the following by just clicking on the title:
Once you have completed the Family Health History you then can proceed to do a Personal Health Appraisal Interview with your client.
You can download the following by clicking on the title
|
Relevant Research Related to ACE Factor
ACE Factor researchers found that children in alcoholic households are more likely to have adverse experiences. They found that the risk of alcoholism and depression in adulthood increases as the number of reported adverse experiences increases regardless of parental alcohol abuse. Depression among adult children of alcoholics appears to be largely, if not solely, due to the greater likelihood of having had adverse childhood experiences in a home with alcohol-abusing parents (Anda, Whitfield, Felitti, Chapman, Edwards, Dube, & Williamson, 2002). In a related study at the time, it was found that early family adversity such as abusive or neglectful parenting can impact cognitive performance in older adulthood through psychosocial, behavioral, and health–related pathways operating across the lifespan (Luecken, 2006). Medical research on “adverse childhood experiences” (ACEs) reveals a compelling relationship between the extent of childhood adversity, adult health risk behaviors, and principal causes of death in the United States (Fielitti & Anda, 2010; Larkin, Flelitti, & Anda, 2014).
ACE Factors researchers found that adults with an ACE score≥ 6 were 5.9 (95% CI, 4.4–7.9) times more likely to have Autobiographical Memory Disturbance (CAMD compared to adults with an ACE score of 0. (Brown, Anda, Edwards, Dube, Giles, 2007). These researchers went on to recommend that it was very appropriate and clinically sound to ask patients about their past (Edwards, Dube, Felitti, & Anda, 2007). These researchers also found that both an emotionally abusive family environment and the interaction of an emotionally abusive family environment with the various maltreatment types had a significant effect on mental health scores of those studied (Edwards, Holden, Anda & Felitti, 2003). A study in Australia at the same time found that childhood domestic adverse experiences had substantial associations with clinically important aspects of personality such as neuroticism and negative affect (Rosenman & Rodgers, 2006).
ACE Factor researchers concluded the number of ACEs has a graded relationship to both lifetime and recent depressive disorders. They concluded that these results suggest that exposure to ACEs is associated with increased risk of depressive disorders up to decades after their occurrence. Early recognition of childhood abuse and appropriate intervention may thus play an important role in the prevention of depressive disorders throughout the life span. (Chapman, Anda, Felitti, Dube, Edwards & Whitfield, 2004). They also found that there was a strong relationship of the ACE Score to increased utilization of psychotropic medications in the adults in their study, which underscored the contribution of childhood experience to the burden of adult mental illness. Moreover, they concluded that the huge economic costs associated with the use of psychotropic medications provide additional incentive to address the high prevalence and consequences of childhood traumatic stressors (Anda, Brown, Felitti, Bremner, Dube, & Giles 2007). Base on the reality that ACEs have negative neurodevelopmental influences that persist over the lifespan research examined the relationship between ACEs and self-reported depression among low-income ethnic minority populations who live in an urban setting. Their findings highlight the importance the prevalence of and risks for multiple types of childhood maltreatment, particularly in the somewhat neglected area of self-reported depression (Waite & Shewokis, 2012).
One of the leading ACE Factor researchers commented on findings in another research (Flaherty, Thompson, Litrownik, Zolotor, Dubowitz, Runyan, English, & Everson, 2009). emphasizing that that adverse childhood experiences are surprisingly common even in the earliest years, and are generally unrecognized, can be identified during childhood by history from children and caretakers, and can start to manifest their damage as ill health and somatization during childhood itself and for this reason these factors provide clear opportunity for early intervention (Felitti, 2009). On the other hand, researchers found that early parental emotional abuse was significantly associated with more sleep complaints in older aged people ages 60 and older because unsupportive interactions with family, friends, significant others, and emotional distress partially explained the association (Poon & Knight, 2011). Research also looked at the correlation of ACE factors with smoking and their findings suggest that for women, current smoking cessation strategies may benefit from understanding the potential role of childhood trauma (Strine, Edwards, Dube, Wagenfeld, Dhingra, Prehan, Rasmussen, McKnight-Eily, & Croft, 2012).
Research into implications of ACE factors and premature death of family members found that family members who experienced any type of ACEs were more likely to have elevated prevalence for premature death relative to those without such experience. The highest risk occurred among those who reported having been physically neglected and living with substance abusing or criminal family members during childhood. A powerful relationship between the number of ACEs and premature mortality in the family was observed for all age groups. Their conclusion was that adverse childhood experiences may be an indicator of a chaotic family environment that results in an increased risk of premature death among family members (Anda, Dong, Brown, Felitti, Giles, Perry, Edwards, & Dube, 2009).
Coates (2010) explored the long-term difficulties experienced by adult victims of child abuse in relation to the neurobiological impacts of child abuse on the child’s developing brain. The impact of child abuse on neuro-endocrine functioning and the structure of the brain, in particular on the amygdala, hippocampus, left hemisphere, and corpus callosum were explored. His recommendation was to focus on breaking the cycle of violence and abuse by helping victims build new and safe social relationships and networks. Teaching effective arousal reduction strategies are vital to successfully transitioning from a ‘‘dangerous world’’ to a world of relative safety. In time, and with dedicated effort, the victim will become re-socialized and new neural pathways will form helping the client to live in ‘‘safety’’ with no difficulty and stress.
In reviewing the impact of ACE Factors on health, researchers found that failures in the development of social and emotional competence during childhood may lead to dysregulated responses to stress and difficulties in social relationships across the lifespan. These researchers found that over time, the cumulative impact of dysregulated stress responses and low social support may increase the risk of mental and physical health problems later in life (Luecken, Roubinov, & Tanaka, 2013). In a large population-based cohort, self-reported adverse life events during the lifespan to be a significant negative predictor of heart rate variability at baseline unfortunately the researchers could not replicate the one significant result at follow-up 2 years later in the same cohort, but the reality is that Adverse Life Events do impact the health of the survivors of these events (Van Ockenbrug, Tak, Bakker, Gans, de Jonge, & Rosmalen, 2015).
Researchers after interviewing over 100 low-income women in Utah found that their early childhood losses undermined the development of personal characteristics and contributed to difficulties in their maintenance or accumulation of resources that may have helped support their development into adulthood (Gringeri & Vogel-Ferguson, 2012)..
In a separate study in Hawaii, researchers found the presence of ACEs among women was indicative of Current Depressive Symptoms (CDS) in adulthood, notably verbal abuse. Further, the risk for CDS increased with the number of ACEs. The concomitant exposure to ACEs and current smoking status or binge drinking did not elevate odds for Current Depressive Symptoms (Remigio-Baker, Hayes& Reyes-Savail, 2014).
In a recent study in Brazil researchers found that Over half of the respondents reported at least one childhood adversity. Only physical abuse was consistently associated with suicide attempts in all subsequent life stages. Among adults 20–29 years of age, the likelihood of a suicide attempt was correlated with parental divorce, whereas suicidal ideation was associated with prior sexual abuse. Among adults over 30 years of age, physical illness and economic adversity emerged as relevant childhood adversities associated with suicide attempts, whereas sexual abuse, family violence, and economic adversity were associated with suicidal ideation. (Coelho, Andrade, Borges, Santana, Viana, & Wang, 2016).
In determining if older adults still remembered adverse childhood experience research interview a group of older adults and found their data revealed two main themes: the inner child of these older adults becomes visible and is a presence through life. The participants’ narratives showed that their understanding of the experiences included both positive and negative feelings, as well as ways to be creative, in which the inner child became visible. The participants’ experiences indicated that the inner child was present throughout the lifespan, was found in challenges that occurred in life, and could turn something bad into something good. However, the presence of the inner child could also be a source for development throughout life and could interfere with the person. The findings from this study point to older persons’ need to be recognized, acknowledged, and understood as a unique person living his or her own life. In addition, dimensions of well-being such as feeling safe, loved, supported, and creating space for fantasy and possibilities can be compared to the physical, mental, social, and existential dimensions of well-being found in WHO surveys and definitions of health. This calls for a holistic approach when caring for older persons (Sjoblom, Ohrling, Prellwitz, & Kostenius, 2016).
|
How to Engage Clients with HIGH ACE Factors
When working with clients with High ACE Scores follow the recommended SAMHSA’s (2104) Six Principles of a Trauma-Informed Approach:
Establish a sense of safety in the environment, between you and the clients, as well as inside of the clients.
Be transparent, share what you as a therapist is doing and why you are doing it to build a trusting relationship.
Use peer support, have your clients connect with others who have had similar life experiences to decrease their sense of isolation.
Identify the cultural context and intergenerational aspects of the clients’ trauma, to increase your sensitivity and deepen the clients’ understanding.
Recognize your clients’ expertise and leadership in the healing process. From day one, make it clear that therapy would be a collaborative process, something you will do together, not something you do to your clients.
Maintain a focus on empowering your clients to make their own choices and to express their voices in every step of the healing process.
REMEMBERING: Adverse childhood experiences or later-life traumas can leave a lasting impact on clients’ lives, but they don’t have to dictate their destinies. People need to understand that they are not broken people, damaged goods, or inherently flawed. Rather, they are affected by past events not of their own choosing. Through this mindset they can begin to write a new narrative, a narrative based on empathy, compassion, acceptance, and nurturing. This is where healing begins.
Substance Abuse and Mental Health Services Administration (SAMSHA). (2014). Trauma-Informed Care in Behavioral Health Services. Treatment Improvement Protocol (TIP) Series 57. HHS Publication No. (SMA) 13-4801. Rockville, MD: Substance Abuse and Mental Health Services Administration.
|
Dealing With Health Risks Arising from ACE Factors
The truth is well documented about the false belief that as long as individuals don’t drink or smoke they can be a doting grandparent living well into their 90’s even though they came from a 6 or higher ACE Factor background. Being a sober non-smoker doesn’t inoculate people from health risks associated with developmental trauma and post-traumatic stress. There are no easy ways to override the long reach of childhood toxic stress, trauma and neglect.
So, is it possible for people with High ACE’s to live a normal life span? Can they reverse the death-disease-despair curse of early adversity? Truth is there is no recipe or formula for those with high ACE scores, since everybody is different and every BODY is different. But there is a an approach which has promising outcomes it is called DINE.
DINE
An approach to health that can be used with patients with High ACES is called DINE.
D - Detox.
I - Inflammation.
N - Nutrition.
E - Energy.
Detox
Detox involves removing health threats such as smoking cigarettes, drug or alcohol abuse, and even food, which many people use food as medicine or a coping mechanism, to either numb or comfort themselves. The Detox model advises most of patients to limit or eliminate dairy and gluten from their diet, no matter whether they’re allergic or not. Doing so, will reduce inflammation in the body and makes people feel better because the immune system and serotonin levels get shot because of dairy or gluten. An alternative suggested is eating as many colors of fresh fruit and vegetables in the rainbow as possible. Also letting go of unhealthy relationships with other people, jobs, situations or environments needs to be addressed as part of this detox approach as well. It helps High ACE folks admit how stressful it had become to live in a stress filled life, some changes, like moving, cause more stress before things improve and this can be more challenging when changing or leaving jobs or relationships too.
Inflammation
It is known that stress is bad whose influence is crucial in disease, and cumulatively – it’s impact is worse. Stress is fine if you’re running from a tiger, but stress isn’t curative. It’s inflammatory. It inflames and attacks the body. For example, not sleeping well can increase cortisol and cortisol being up all the time is very inflammatory on the body. Studies have shown C-reactive protein (CRP) increases after major life stressors. To assess cardiac health and inflammation, the CRP level needs to be evaluated. CRP is often elevated, for individuals with high ACES, given their childhood adversity and major adult stressors such as divorce, single parenting and surviving natural disasters. Use of an anti-inflammatory, can help these patients be happy on a regular basis. Daily joy might mean meditation for some or painting the toe nails for others. Holistic approaches that have been recommended acupuncture and Reiki in addition to anti-inflammatory supplements for those with high CRP levels.
Nutrition
For good nutrition, follow this simple bit of advice: Eat as many foods with a sticker UPC code on them — like apples and peppers have — as possible. The suggestion then is to shop the perimeters of grocery stores where food is fresh which is ideal. Some recommendations are: Vitamin D supplements at a high dose (5000 iu daily with food), magnesium (in powder form, at night, 175 to 350 mg. daily) and iron (with organic beet root, twice a day with Vitamin C) to counter lower levels in one’s blood. The magnesium is meant to improve sleep and reduce anxiety. Also recommended are daily fish oil supplements as well as primrose oil.
Energy
Energy means moving energy with exercise and physical activity, as well as working with the energy system as is done with techniques such as acupuncture, body work and with spirituality. Energy the “fourth leg of a healthy table” that stabilizes the system so it’s less likely to tip. The types of energy work recommended for people to use at home are meditation, journaling, HeartMath, (a type of biofeedback which can be done online or on smart phone 5 to 10 minutes a day), as well as walking and yoga. Aces story journaling, hypnotherapy and psychotherapy. Prolonged Exposure Therapy, Cognitive Processing Therapy and EMDR are ways suggests to help balance energy after trauma. These PTSD treatments are ways to pull (trauma) out and dump it instead of carrying it in the bod. Also suggested are a daily gratitude list or journal before bed so people are shutting down with the positive each night. This practice can increase levels of happiness in three to six months. There’s a lot of research that journaling is very therapeutic. A three-page writing habit each morning with page one used to dump stress, page two listing things to look forward to and the third page detailing what one is thankful for.
|
In addition to the ACE Factors Assessment, Assess Client's Resilience
To find out if a person has Protective Factors/Positive Role Models in and Outside of the family consider using this assessment:
A good overview of these two measures is at: https://acestoohigh.com/got-your-ace-score/
|
Resilience/Stress Questionnaire
Name ___________________________________________ Date: ______________
Your answers are confidential. You do not need to share them with anyone but you may find it helpful to do so. If answering any of the questions is disturbing, you may answer them at another time if you prefer.
Directions: Put in the number for the answer which is most accurate on the line before the item:
1 = Definitely True
2 = Probably True
3 = Not Sure
4 = Probably Not True
5 = Definitely Not True
_____1. I believe that my mother loved me when I was little.
_____2. I believe that my Father loved me when I was little.
_____3. When I was little, other people helped my mother and father take care of me and they seemed to love me.
_____4. I’ve heard that when I was an infant someone in my family enjoyed playing with me and I enjoyed it too.
_____5. When I was a child, there were relatives in my family who made me feel better if I was sad or worried.
_____6. When I was a child, neighbors or my friends' parents seemed to like me.
_____7. When I was a child, teachers, coaches, youth leaders, or ministers were there to help me.
_____8. Someone in my family cared about how I was doing in school.
_____9. My family, neighbors and friends talked about making our lives better.
_____10. We had rules in our house and were expected to keep them.
_____11. When I felt really bad, I could almost always find someone I trusted to talk to
_____12. As a youth, people noticed that I was capable and could get things done
_____13. As a youth, I was independent and a go-getter.
_____14. As a youth, I believed that life is what you make it.
Once you have answered the 14 items then answer the following:
_____How many of the fourteen items, known as protective factors did I rate as Definitely True or Probably True that I had as a child and youth?
_____Of those Definitely True or Probably True, how many are still true for me today?
Please share positive memories about situations that you feel have increased your ability to handle adversity? (Please Explain):
|
Albert Bandura’s Self-System Explains How Folks Survive ACE Factors in their lives
Bandura's Self System was developed over the years from 1957-1997. His model describes how people develop their personality through a set of cognitive processes by which they perceive, evaluate, and regulate personal behavior so that it is appropriate to the environment and effective in achieving their individual goals.
Relevant to ACE factors is the concept of Observational Learning. Bandura believed that:
Observational learning + inner person + demands of situation combine to determine behaviors.This allows for the cognitive process to mediate between environment and behavior
Bandura believed that people cognitively represent the behavior of others and then sometimes adopt this behavior themselves. His model shows a reciprocal influence of behavior, personal and cognitive factors, and environment.
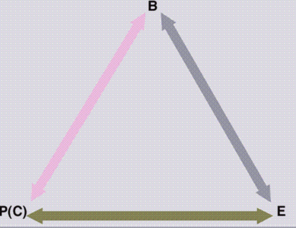
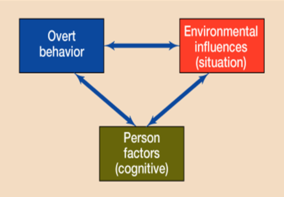
Bandura develop a model of Reciprocal Influence:
B = Behavior
P(C)= Personal & Cognitive Factors (such as intelligence, skills & self-control)
E = Environment (Protective Factors)
The arrows reflect how relations between these factors are reciprocal rather than unidirectional.
|
What is Observational Learning?
It is how new behaviors are acquired in absence of reinforcement. In other words, Observational learning is vicarious learning gained second hand by watching the experience of another. Another way of looking at it, it is Modeling where a person forms self in image of another.
It is based on Outcome Expectancy which is that the expected consequence of the behavior is most significant influence on whether an observer will reproduce an observed behavior. Individuals are more likely to imitate behavior that they believe leads to positive outcomes. Outcome expectancy is based on both consequences of rewards and punishments and on anticipated consequences.
The Four Components of Observational Learning are:
- Attention: influenced by characteristics of the model & situation
- Retention: influenced by cognitive ability of observer and ability to encode the behavior-images or verbal representation
- Motor reproduction: turn mental representation into physical action-mentally rehearse the behavior
- Motivation: most influences actual performance of the behavior which has been observed-valued vs negative outcomes
|
What are the Outcomes of Observational Learning from Positive Role Models?
Here are some of the benefits of Observational Learning
1. Self Regulation
Individual’s internal processes of goals, planning, & self-reinforcement result in self-regulation of behavior
Self-punishment: feelings of self-disgust, shame or withhold desired object
Internal standards used to measure own success or failure-gained by both observation and past behavior acting
2. Self-Efficacy
An expectancy or belief (expectation) about how competently one will be able to enact a behavior in a particular situation
Positive: belief will be able to perform
Determines: if we try, how long we persist, how results influence future behavior
Self-Efficacy Results from 4 types of Information
- Experience: trying to perform the behavior with resulting failure or success in the process
- Watching: observing others performing the same or similar behaviors vicariously
- Verbal Persuasion: being given encouragement from others on the quality of the behaviors exhibited
- Emotional Reaction: How individual feels about performing the given behaviors based on the feedback from self and others
3. Resilience
Resilience is the ability to absorb failure and disappointment and still believe in oneself. It is the ability to take the hard knocks and survive to be justified by success in one’s life. It is the stuff that overcomes adversity. It is the bolstering one’s self-efficacy against all types of challenges to succeed in the end. Thus the reason why many people with high number of ACE Factors in their lives succeed in life despite them.
|
Adverse Childhood Experiences Reference
Anda, R.F., Brown, D.W., Felitti, V.J, Bremner, J.D., Dube, S.R., & Giles, W.H. (2007) Adverse childhood experiences and prescribed psychotropic medications in adults. American Journal of Preventive Medicine, 32(5), 389–394.
Anda, R.F., Dong, M., Brown, D.W., Felitti, V.J., Giles, W.H., Perry, G.S., Edwards, V.J., & Dube, S.R. (2009). The relationship of adverse childhood experiences to a history of premature death of family members. BMC Public Health 9, 106. doi:10.1186/1471-2458-9-106
Anda, R.F., Whitfield, C.L., Felitti, V.J., Chapman, D., Edwards, V.J., Dube, S.R., & Williamson, D.F. (2002). Adverse childhood experiences, alcoholic parents, and later risk of alcoholism and depression. Psychiatric Services, 53(8),1001–1009.
Brown, D.W., Anda, R.F., Edwards, V.J., Felitti, V.J., Dube, S.R., & Giles, W.H. (2007). Adverse childhood experiences and childhood autobiographical memory disturbance. Child Abuse & Neglect, 31, 961-969.
Chapman, DP, Anda, RF, Felitti, VJ, Dube, SR, Edwards, VJ, & Whitfield, CL. (2004). Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Affective Disorders, 82, 217–225.
Coates, D. (2010). Impact of childhood abuse: Biopsychosocial pathways through which adult mental health is compromised. Australian Social Work, 63(4), 391-403. DOI: 10.1080/0312407X.2010.508533
Coelho, B.M., Andrade, L.H., Borges, G., Santana, G.L., Viana, M.C., & Wang, Y.P. (2016). Do childhood adversities predict suicidality? Findings from the general population of the metropolitan area of San Paulo, Brazil, PLOS ONE, DOI:10.1371/journal.pone.0155639
Edwards, V.J., Dube, S.R., Felitti, V.J., & Anda, R.F. (2007). It's OK to ask about past abuse. American Psychologist, 62(4), 327–328.
Edwards, V.J., Fivush, R., Anda, R.F., Felitti, V.J., & Nordenberg, D.F. (2001) Autobiographical memory disturbances in childhood abuse survivors. In: J.J. Freyd and A.P. DePrince (Eds.) Trauma and Cognitive Science: A Meeting of Minds, Science, and Human Experience. Binghamton, NY: Haworth Press.
Edwards, V.J., Holden, G.W., Anda, R.F., & Felitti, V.J. (2003) Experiencing multiple forms of childhood maltreatment and adult mental health in community respondents: results from the Adverse Childhood Experiences (ACE) Study. American Journal of Psychiatry,160(8), 1453–1460.
Felitti, V.J. (2009). Adverse childhood experiences and adult health. Academic Pediatrics, 9(3), 131-132.
Feliitti, V.J., Anda, R.F., Nordenberg, D., Williamson, D.F., Spitz, A.M., Edwards, V., Koss, M.P., & Marks, J.S. (1998). Relationship of childhood abuse and household dysfunction to many to many of the leading causes of death in adults – The adverse childhood experiences (ACE) study. American Journal of Preventative Medicine, 14(4), 245-258.
Felitti, V.J. & Anda, R.F. (2010). The relationship of adverse chlldhood experiences to adult medical disease, psychiatric disorders and sexual behavior: Implications for healthcare. In Lanius, R.A., Vermetten, E & Pain, C.(Eds.). The impact of early life trauma on health and disease: The hidden epidemic. Cambridge, England: Cambridge University Press
Flaherty, E.G., Thompson, R., Litrownik, A.J., Zolotor, A.J., Dubowitz, H., Runyan, D.K., English, D.J., & Everson, M.D. (2009). Adversé childhood exposures and reported child health at age 12. Academic Pediatrics, 9, 150-156.
Gringeri, C. & Vogel-Ferguson, M.B. (2012). Childhood abuse and lose in the lives of low-income women. Qualitative Social Work, 12(5), 654-670. DOI: 10.1177/1473325012451481
Larkin, H., Felitti, V.J., & Anda, R.F. (2014). Social work and adverse childhood experiences research: Implications for practice and health policies. Social Work in Public Health, 29, 1–16. DOI: 10.1080/19371918.2011.619433
Luecken, L.J. (2006). Early family adversity and cognitive performance in aging: A lifespan developmental model. Journal of Social and Clinical Psychology, 25(1), 33-52.
Luecken, L.J., Roubinov, D.S., & Tanaka, R. (2013). Childhood family environment, social competence, and health across the lifespan. Journal of Social and
Personal Relationships, 30(2), 171–178. DOI: 10.1177/0265407512454272
Poon, C.Y. & Knight, B.G. (2011). Impact of childhood parental abuse and neglect on sleep problems in old age. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences,66(3), 307–310. doi:10.1093/geronb/gbr003.
Remigio-Baker, R.A., Hayes, D.K., & Reyes-Savail, F. (2014). Adverse childhood events and current depressive symptoms among women in Hawaii: 2010 BRFSS, Hawaii. Maternal and Child Health Journal,18(10), 2300-2308. doi: 10.1007/s10995-013-1374-y.
Rosenman, S. & Rodgers, B. (2006). Childhood adversity and adult personality. Australian and New Zealand Journal of Psychiatry, 40, 482–490.
Sjoblom, M., Ohrling, K., Prellwitz, M., & Kostenius, C. (2016). Health throughout the lifespan: The phenomenon of the inner child reflected in events during childhood
experienced by older persons. International Journal of Qualitative Studies on Health and Well-being, 11. http://dx.doi.org/10.3402/qhw.v11.31486
Strine, T.W., Edwards, V.J., Dube, S.R., Wagenfeld, M., Dhingra, S., Prehan, A.W., Rasmussen, S., McKnight-Eily, L. & Croft, J.B. (2012). The mediating sex-specific effect of psychological distress on the relationship between adverse childhood experiences and current smoking among adults. Substance Abuse Treatment, Prevention, and Policy. Retrieved at: http://www.substanceabusepolicy.com/content/7/1/30
Van Ockenbrug, S.L., Tak, L.M., Bakker, S.J.L., Gans, R.O.B., de Jonge, P., & Rosmalen, J.G.M. (2015). Acta Psychiatrica Sandinaavica, 131, 40-50. DOI: 10.1111/acps.12286
Waite, R. & Shewokis, P.A. (2012). Childhood trauma and adult self-reported depression. Association of Black Nursing Faculty Journal (ABNF), 23 (1), 8-13.
|
References for Bandura's Self-System
- Bandura, A., & Walters, R. H. Adolescent aggression. New York: Ronald Press, 1959.
- Bandura, A., & Walters, R. H. Social learning and personality development. New York: Holt, Rinehart & Winston, 1963.
- Bandura, A. Principles of behavior modification. New York: Holt, Rinehart & Winston, 1969.
- Bandura, A. (Ed.). Psychological modeling: Conflicting theories. Chicago: Aldine-Atherton Press, 1971.
- Bandura, A. Aggression: social learning analysis. Englewood Cliffs, N.J.: Prentice-Hall, 1973.
- Bandura, A. Social learning theory. Englewood Cliffs, N.J.: Prentice-Hall, 1977.
- Bandura, A. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, N.J.: Prentice-Hall, 1986.
- Bandura, A. (Ed.). Self-efficacy in changing societies. New York: Cambridge University Press, 1995.
- Bandura, A. Self-efficacy: The exercise of control. New York: Freeman, 1997
|
|
|