Tools to Assist Recovery from Alcohol/Substance Use
Recovery Language
Restructuring Thoughts
Behavioral Chains
Thought Stopping
Handling Cravings
Refusal Skills
|
|
Treatment for Alcohol & Substance Use Disorders A Training Resource
By Jim Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
Types of Therapy for Drug and Alcohol Addiction
This article covers the following issues:
NOTE: We are grateful to Mr Michael Waters and one of his students Jeremy for referring this wonderful resource to our website.
|
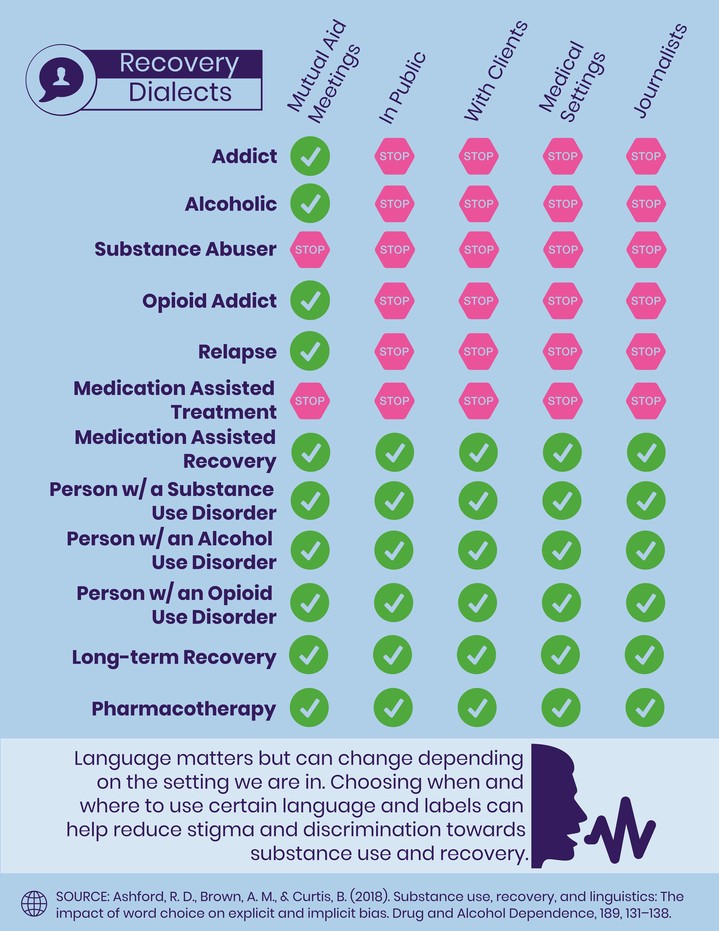
Need to Change Terminology in the World of Substance and Alcohol Recovery
Addiction researchers at the University of Pennsylvania say it’s time to stop using “addict” and “alcoholic” when talking about people with substance use disorders (Ashford, Brown & Curtis, 2018). The recommendation comes out of a new study that found the terms are associated with a strong negative bias.
|
These researchers’ goal was to study the belief that the general public, treatment professionals, and healthcare professionals have been found to exhibit an explicit negative bias towards substance use and individuals with a substance use disorder (SUD). They were also studied terms such as “substance abuser” and “opioid addict” which had been shown to elicit greater negative explicit bias. They also wanted to explore other common terms which had not yet to be empirically studied.
1,288 participants were recruited from ResearchMatch. Participants were assigned into one of seven groups with different hypothesized stigmatizing and non-stigmatizing terms. Participants completed a Go/No Association Task (GNAT) and vignette-based social distance scale. Repeated-measures ANOVAs were used to analyze the GNAT results, and one-way ANOVAs were used to analyze vignette results.
|
The terms “substance abuser”, “addict”, “alcoholic”, and “opioid addict”, were strongly associated with the negative and significantly different from the positive counter terms. “Relapse” and “Recurrence of Use” were strongly associated with the negative; however, the strength of the “recurrence of use” positive association was higher and significantly different from the “relapse” positive association. “Pharmacotherapy” was strongly associated with the positive and significantly different than “medication-assisted treatment”. Both “medication-assisted recovery” and “long-term recovery” were strongly associated with the positive, and significantly different from the negative association.
Results of this study support calls to cease use of the terms “addict”, “alcoholic”, “opioid addict”, and “substance abuser”. Additionally, it is suggested that “recurrence of use” and “pharmacotherapy” be used for their overall positive benefits. Both “medication-assisted recovery” and “long-term recovery” are positive terms and can be used when applicable without promoting stigma.
Reference:
Ashford. R.D., Brown, A.M. & Curtis, B. (2018). Substance use, recovery, and linguistics: The impact of word choice on explicit and implicit bias. Drug and Alcohol Dependence, 189, (1 August 2018), 131-138. https://doi.org/10.1016/j.drugalcdep.2018.05.005
|
Thought Restructuring
Common Thoughts Associated with alcohol and/or substance use disorder
- Testing control: “I can go to parties(see friends who are users, drink, or smoke pot) without using.”
- Life will never be the same: “I love being high!”
- Failure: “Previous treatments and efforts to change my habits haven’t worked; there’s no hope for me.”
- Diminished pleasure: “The world is boring without alcohol or drugs.”
- Entitlement: “I deserve a reward so I am going to get high.”
- Feeling uncomfortable: “I don’t know how to be with people if I’m not high.”
- What’s the use of trying: “I screwed up again, I might as well get high.”
- Escape: “My life is so bad, I just need a break for a few hours.”
How to counter thoughts which lead to a person to alcohol and/or substance use disorder
People can:
- Think of unpleasant aftermath of highs they get when they use
- Challenge the thoughts with an alternative thought-use humor and reframing
- Review negative consequences to counter the urging and craving to use
- Use distracting pleasant activities to prevent their going back to using
-
Seek out a supportive friends who are understanding so as to pinpoint steps they need to take to not use again
-
Keep a journal of their thoughts, feelings and reactions to people, places, situations and conditions so that they can identify if theyare building up to going back to their old pattern of substance use or abuse
Journal writing helps people plan their recovery from alcohol and/or substance use disorders
In a journal people can record the following:
- Changes I will make while focused on recovery:
- Reasons why I want to make these changes:
- Steps I plan to take to make these changes:
- Ways other people can help me make changes:
- Things which might interfere with my change plan:
In the Journal people can keep track of their thoughts about alcohol and/or substances
Thoughts about alcohol & drugs I have:
1
2
3 etc
Positive thoughts and coping skills used to counter these thoughts:
1
2
3 etc
In Journal people can write about the people who are involved in their use of alcohol and/or substances
People can list the following:
Person who get high with me on my alcohol and/or drug outings:
1
2
3 etc.
Then for each person listed, people can answer the following:
Write an honest statement as to how good this person is for me to hang out with, in my recovery
1
2
3 etc.
In Journal people can write about non-use Alternative Activities to do
Old Activities I did which led to alcohol and/or Substance use:
1
2
3 etc.
New Activities I will do which will prevent my alcohol and/or Substance use:
1
2
3 etc.
|
Behavioral Chains
Use Behavioral Chains in Recovery
Behavioral Chains are:
- Series of specific behaviors resulting in a final behavior in need of attention, remediation, or change before a recovered lifestyle can be achieved or regained
- Steps leading to a behavior targeted for change or relapse prevention work.
- Series of stimuli/response reactions, ultimately leading to a problem behavior or relapse event.
- Specific behavior traits that make up and are the causal agents of a problem behavior pattern when linked together.
- Linked behavior traits with some degree of predictability as to the ultimate consequence or outcome.
- The result of linking emotional cues and respondent behaviors into a series of events that contribute to the exacerbation of problem behavior patterns or relapse of this pattern
Characteristics of Behavior Chains
- If the chain of behavior patterns is broken at any point, it probably will not progress to the final behavior.
- The earlier the break in the link, the easier it is to undo the chain.
- Behavior chains often go unidentified prior to the occurrence of the final link in the chain.
- Behavior chains are self‑propelling; they have a momentum of their own to go on and on.
- The chains can be diagramed, but one must begin with the last link and trace backward to each preceding behavior or emotional cue.
- Behavior chains can be broken into habitual patterns that give insight into chain‑breaking strategies and alternative behavior traits which help to prevent future relapse.
Sample of a Behavioral Chain
(Remember the identifying of this behavioral chain began at the bottom of the list with the relapse event and then the person was asked what happened before that step until the person has exhausted the steps which led to the relapse event)
The Beer Relapse:
- You have had a horrible day at work and are feeling pressured by your boss to either increase daily quota of work or face poor performance evaluation.
- You leave work in distress, upset over not having been assertive, not standing up for your rights with the boss.
- In the heavy commuter traffic, you feel upset over course of the day.
- Driver in the car next to you cuts in front of you, making you shout and gesture to him.
- You pass several bars and think of a big, cool beer.
- You honk horn loudly at driver in front of you who has slowed down the pace of traffic.
- Angry at self for losing temper.
- See billboard with a local watering hole advertised.
- You feel the seat belt pressing in on your stomach and you think more about your thirst and desire for a beer to quench that thirst.
- Depressed over your boss's inability to show appreciation for your good work.
- Annoyed at the slow pace of traffic.
- Getting angry and tasting the beer as you pass the twelfth bar.
- Finally you pull into a bar parking lot.
- You call home to say you will be late, that you have more work to do at the office.
- Check your wallet to see if you have enough money for a beers.
- Angry at self for allowing work, boss, and traffic to upset you.
- Get into bar and stand at the bar counter.
- Feel exhilarated when it is your turn to order.
- Order a large, cool tap beer.
- Mentally review the day's events as you wait for your beer to come.
- Get angry again over your boss's rudeness and lack of caring.
- You feel depressed as you review the route your life has taken: overworked, underappreciated, and taxed by a forty‑five minute commute twice a day.
- Feeling sorry for self for the hard knocks life has dealt you.
- Your bottle of beer arrives and you feel excited over your rewarding of yourself; you deserve it!
- Pay for beer and become intoxicated by the aroma.
- You drink your first slug of beer.
- You take a deep breath, feeling rewarded and at peace.
- You continue to drink slug after slug of your beer and relish each flavor.
- You force yourself to order another beer.
- You feel after the second beer is guzzled down, embarrassed: What have you done! Why did you drink two beers?
- Guilty and depressed since you have been in treatment for alcohol use disorder, you dispose of all evidence that you were at the bar.
- You drive home feeling hopeless, trapped. Why did you lie about doing work at the office when you were going for two beers? Why did you drink? Why did you threaten your recovery. You hate yourself.
- You know you need to bring this up to your AA Sponsor and maybe even talk about this relapse event in your AA meeting tomorrow night.
How can people control a behavioral chain?
In order to control a behavioral chain, the links need to be identified and broken.
People can work at:
- Interpreting events in one’s life differently so that they are less likely to have the power to lead them to exercise habitual problem behavior or relapse to old behaviors.
- Using rational thinking about what is happening in one’s life eliminates the "shoulds'' and "musts'' from peoples’ thinking about how others should treat them and how they should treat others.
- Substituting positive affirmations and positive self‑talk when people are being bombarded with emotional cues or irrational thoughts about themselves, events, or others.
- Taking responsibility for their own actions, not blaming other persons or events for making them fall into the behavior chain.
- Substituting alternative, healthy behavior, for those behavior traits that lead to the problem behavior or relapse event.
- Substituting required activities for antecedent behavior in a chain, such as doing office work, paying bills, cleaning the house, opening the mail, paying attention to defensive driving techniques, etc.
- Substituting enjoyable activities for antecedent behaviors in a chain such as enjoying a hobby, listening to music, exercising, calling a AA or NA Buddy, writing a letter, going to a movie, reading for pleasure.
- Substituting positive behavior in a chain of behavior known to lead to habitual problems or relapse events.
- Reinforcing positive behavior traits and ignoring negative behavior patterns, or substituting new behavior traits for negative behavior patterns or relapse events.
- Recognizing the behavior that habitually leads to predictable, negative‑consequence behavior chains or relapse events.
What beliefs block people from recognizing the behavioral chains in their problem behavior patterns?
- I never know why I do the things I do. It's beyond me.
- There is no sense in looking at the causes of my behavior. What's important is to treat the symptoms.
- I've always done it this way. I will never change.
- What difference does it make what behavior preceded my problem behavior? All I know is I have a problem I can't seem to shake.
- It takes too much time to work on analyzing the chain of events leading to my problem behavior.
- So, what difference will it make to identify antecedent behaviors or events when they are out of my control anyway?
- I'm compulsive; that's all I need to know to explain why I act the way I do.
- I'm so embarrassed by the way I act; I'd hate to tell anybody else about it.
- I am a loser and there is no helping me.
- If it weren't for ________ (spouse, parent, child, boss, job, problem of the day), these things would never happen.
|
Thought Stopping for Recovery
What is thought stopping?
Thought stopping is the:
- Process by which people are able to cease dwelling on a thought bothersome to them
- Procedure used to stop thoughts that are cues to acting impulsively or compulsively
- Process by which people are able to break the power of the cues that lead you into addictive binge‑like or relapse behaviors
- Substitution of a healthy thought for an unhealthy thought
- Act of deliberately turning to cues that break unhealthy patterns or habits.
- Ability to discontinue obsessing on an idea, image, thought, fear or stimuli that is a cue for unhealthy behavior
- Practice of using mental energy in a positive way
- Technique used to reduce the negative impact of stress, unhealthy emotional cues, and fears
- Stress‑reduction technique that eliminates the overwhelming impact of stress and/or crisis events
How does thought stopping work?
In thought stopping people:
- Replace one thought for another, i.e., the thought of drinking is replaced by the thought of exercising
- Hear “stop'' literally or figuratively whenever a negative or unhealthy thought arises, e.g., the desire for a beer appears and “stop'' is immediately heard
- Are able to break an obsessive, unhealthy thought pattern by substituting a healthy thought pattern
- Are able to replace a negative or unhealthy image with a positive visual image
- Can divert or detour their minds from unhealthy or negative thoughts
- Can clear minds of all unnecessary and unhealthy thoughts that create stress or cues for acting out in unhealthy ways
What are some thought‑stopping techniques?
- Thought Replacement: when an unwanted thought enters, immediately replace the thought with a healthy, rational one
- Yelling “Stop”: on thinking the unwanted thought, immediately yell STOP. The yell can be out loud or only in the mind. Continue to yell STOP until the unwanted thought ceases.
- Substituting a Healthy Thought Pattern: if people have a tendency to think irrationally due to irrational beliefs, they can develop a rational pattern of thinking by challenging every thought that comes to mind, asking: Is this a rational thought? If not, what is irrational about it? What would be a rational replacement for this thought?
- Replacement Visual Image: if people have a tendency to visualize negative images, replace these negative images by positive, healthy images.
- Aversive Replacements: if people have a tendency to think of an unhealthy behavior in an acceptable manner, immediately replace these acceptable images with more honest images, i.e., thoughts of beer can be replaced by the words “poison,'' “unhealthy,'' “disgusting,'' “barf'‘ “coffin nails'' or “killers.''
What irrational beliefs block people from letting thought stopping work for them?
- It's OK if I just think about it and do nothing about it.
- What's the harm of thinking about it?
- People will never know if I just think about it for a little while.
- I've denied myself so much, why can't I just think about it once in a while?
- You can't condemn me for thinking.
- I never thought about it before I acted so why should I avoid thinking about it now?
- It is too much of a battle to fight these thoughts. It's easier to give in and then start over again in the morning.
- What difference does it make if I think about it?
- It seems so silly to control my mind from having thoughts about it.
- This feels like brainwashing and I think brainwashing is bad.
- I don't have time to do this.
- I don't need this in order to be successful in achieving recovery.
- This is another far‑out psychological gimmick too stupid to try.
Directions for "Yelling Stop" Thought Stopping
Step 1: Use relaxation training and breathing exercises to get yourself relaxed. It is important that you be relaxed as you proceed with this process.
Step 2: Record the word stop in alternating 1, 2, and 3‑minute intervals on a 30‑minute recording session. Using the stop recording in a relaxed state, think your unwanted thought and every time you hear stop, discontinue the thought. Go back to the thought again and cease the thought only when you hear stop. Do this for 30 minutes every night for two weeks or until you can consistently discontinue the thought when you hear stop.
Step 3: After you are trained to arrest your thought using the stop recording, you are ready to try arresting your thought by yelling stop out loud. Think of your unwanted thought for 30 minutes and yell stop to discontinue the thought. Once you arrest the thought, go back to thinking about it for a while, then yell stop again. Do this for 30 minutes each night for two weeks or until you are able to consistently discontinue the thought by yelling stop.
Step 4: After you have trained yourself to stop thoughts by yelling stop, you are ready to train your thoughts to end by whispering stop. For thirty minutes, repeat the process of dwelling on your unwanted thoughts but this time whisper stop to halt them. Do this 30 minutes nightly for two weeks or until you are able to consistently discontinue the thought by whispering stop.
Step 5: After you have trained yourself to discontinue unwanted thoughts by whispering stop, you are ready to train your thoughts to discontinue by thinking the word stop. Repeat the process of dwelling on your thought for 30 minutes, but this time simply think stop to discontinue unwanted thoughts. Do this for 30 minutes nightly for two weeks or until you are able to consistently discontinue unwanted thoughts by thinking the word stop.
The technique of either recording, yelling, whispering, or thinking stop can be effective in discontinuing unwanted thoughts. Ideally you could get to the point where simply thinking stop would work; however, use whichever mode works best for you and keep practicing.
Remember to start the process in a relaxed state.
|
Handling Cravings
Cravings and Urges to Use Alcohol and Substances
- Urges are common and normal
- They are not a sign of failure
- One can learn from them about what your craving triggers are
- Urges are like ocean waves
- They get stronger only to a point, then they start to go away
- If one doesn’t use alcohol or drugs, one's urges will weaken and eventually go away
- Urges only get stronger if one gives in to them
- People can try to avoid urges by avoiding or eliminating the cues that trigger them
Handle Cravings and Urges
People can:
- Distracting themselve for a few minutes
- Talking about the urge with someone supportive
- “Urge surfing” or riding out the urge
- Recalling the negative consequences of using
- Talking themselves through the urge
In Journal keep record of daily cravings and urges
Date / Time
Situation
Intensity of Cravings (0-100)
Length of time of Craving
How I coped
Refusal Skills
In refusing alcohol or drugs
People need to:
- Respond rapidly (not hemming and hawing, not hesitating)
- Have good eye contact
- Respond with a clear and firm “no” that does not leave the door open to future offers of alcohol or drugs
How to say no without guilt or feeling uncomfortable
When people say “no” it can be followed by:
- changing the subject
- suggesting alternative activities
- clearly requesting that the individual not offer alcohol or drugs again in the future. (“Listen, I’ve decided to stop using and I’d like you not to ask me to use with you anymore. If you can’t do that, I think you should stop coming over to my house.”)
Unhealthy and unproductive decisions common among alcohol and substance users
- Using any alcohol, marijuana, or other drugs other than their drug of choice
- Keeping alcohol in the house
- Not destroying drug paraphernalia
- Going to parties where alcohol or drugs might be available
- Interacting with people who are alcohol and drug abusers
- Keeping past drug and alcohol abuse a secret from family members
- Not telling alcohol or drug-abusing associates of the decision to stop
- Not planning to fill free time
- Having a lot of unscheduled time on nights or weekends that can lead to boredom
- Getting overtired or stressed
Managing Contact with Alcohol and Other Substances at Home
People can record in their "Recovery Journals:"
- Source of Alcohol or Drugs
- Steps I’ll take to reduce availability
Tips for responding to offers of alcohol or drugs
People can:
- Say “no” first
- Make direct eye contact
- Ask the person to stop offering
- Don’t be afraid to set limits on contact
- Don’t leave the door open to future offers (e.g.”not today...”)
Assertive Refusals
People can use the following ty;es of assertive approaches:
- Assertive: uses “I statements” to let the other understand their feelings about the situation, circumstances and behaviors of the other
- Assertive: standing up for their rights
- Assertive: taking risk that is not ruled by fear of rejection or disapproval
- Assertive: rational belief-”I deserve to stand up for my rights.”
Practice in Journal Refusal Skills
People in their journals can practice refussal skills by writing out examples of what they would say or do using the following scenerios:
- A friend with whom they used to use
- A family member with whom they used to use
- At a party
- With their gang of associates
- An associate at work or school
- Their significant others
If people run into a high-risk situation
- They will leave or change the situation
- They will identify safe places for themselves
- They will put off the decision to use for 15 minutes. Realizing that cravings go away forthem in ___ minutes
- They will distract themselvesf with something they like to do
- They will call their emergency backups
- They will challenge Their thoughts about using with positive thoughts
|
|
|