Unit 3: Initial Engagement in
Treating a Suicidal Client
|
|
Suicide Intervention and Prevention Strategies - A Training Resource By: Jim Messina
|
|
|
Basic Intervention Steps
Three basic steps:
1. Show you care
2. Ask about suicide
3. Get help
1. Show You Care
Take ALL talk of suicide seriously. If you are concerned that someone may take their life, trust your judgment.
Listen carefully.
Reflect what you hear.
Use language appropriate for the age of the person involved
Be Genuine
- Let the person know you really care!!!
- Talk about your feelings and ask about his or hers.
2. Ask about suicide
Don’t hesitate to raise the subject.
Be direct, but non-confrontational. Engage them:
- Are you thinking about suicide?
- What thoughts or plans do you have?
- Are you thinking about harming yourself, ending your life?
- How long have you been thinking about suicide?
- Have you thought about how you would do it?
- Do you have _____ (Insert means, weapon, etc.)
- Do you really want to die, or do you want the pain to go away?
Ask about Treatment
- Do you have a therapist/doctor?
- Are you seeing him/her?
- Are you taking your medications?
3. Get Help
- Do not leave the person alone
- Know referral resources
- Reassure the person
- Encourage the person to participate in the helping process
- Encourage the suicidal person to identify other people in their lives who can also help.
Outline a safety plan:
- Make arrangements for the helper to come to you OR take the person directly to the source of help. Once therapy (or hospitalization) is initiated, be sure the suicidal person is following through with appointments and medications.
|
A Hierarchical Approach to Exploring Suicidal Thoughts and Intent
Step 1: Is the client having suicidal thoughts?
Step 2: Reduce resistance and anxiety surrounding suicidal thinking by exploring client's suicidal history before examining the current episode in detail.
Step 3: Transition back to the current suicidal crisis.
Assess specificity of thinking including Frequency, Intensity, Duration, including access. You can use the acronym, F-I-D.
Step 4: Assess subjective intent, including reasons for dying
Step 5: Assess objective intent:
Step 6: Assess protective factors, including reasons for living.
|
What works in Treating Clients to Prevent Suicidal Thinking and Actions
What works? (Rudd, Williamson, & Trotter, 2009).
1. Theoretical models easily translated to clinical work
2. Treatment fidelity
3. Adherence
4. Emphasis on skills-building
5. Personal responsibility
6. Easy access to treatment and crisis services
1. Theoretical models easily translated to clinical work
- Well-defined and theoretical models embedded in empirical research
- Identify thoughts, emotional processing, and associated behavior responses
- Clients can easily understand why they have tried or are thinking about suicide
2. Treatment fidelity
- Clinician training to competence with supervision
- Manual-driven
- Clear sequence or hierarchy of treatment targets
- Suicidal behaviors is central treatment focus independent of psychiatric condition
3. Adherence
- Specific interventions and techniques to target poor adherence and motivation
- Clear directions about what to do if nonadherence emerges
4. Emphasis on skills-building
- Identification of skills deficits with opportunity for skills building and practice
- Clear understanding of “what is wrong” and “what to do about it”
5. Personal responsibility
- Emphasis on client self-reliance and self-management
- Clients assume high level of responsibility for their care, including crisis management
6. Easy access to treatment and crisis services
- Clear plan of action for emergencies
- Dedication of time to practicing skills necessary to identify true crisis, using crisis plan, and using external support services judiciously
|
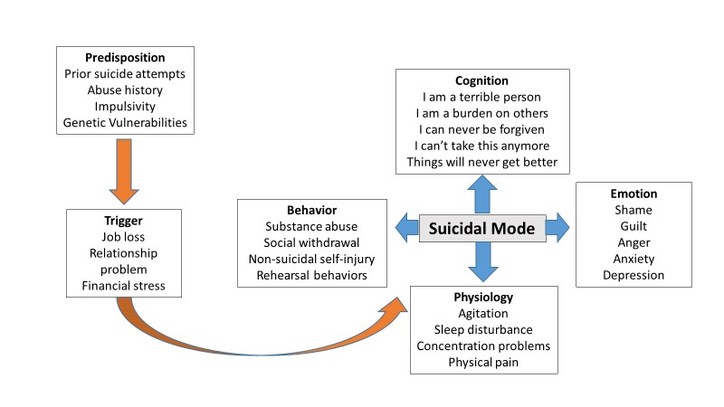
Functional Model of Suicide
|
|
Positive Reinforcement
|
Negative Reinforcement
|
|
Automatic
(Internal)
|
Adding something desirable
“To feel something, even if it is pain.”
|
Reducing Tension or
Negative Stress
“To stop bad feelings.”
|
|
Social
(External)
|
Gaining something from others
“To get attention, to let others know how I feel.”
|
Escape interpersonal task demand
“To avoid punishment from others or avoid doing something undesirable.”
|
|
Fluid Vulnerability Theory
Fundamental Assumptions:
- Baseline risk varies from individual to individual
- Baseline risk is determined by static factors
- Baseline risk is higher and endures longer for multiple attempters (2 or more attempts)
- Risk is elevated by aggravating factors
- Severity of risk is dependent on baseline level and severity of aggravating factors
- Risk returns to baseline level only
- Risk is reduced by protective factors
- Multiple attempters have fewer available protective factors (support, interpersonal resources,
- Risk is elevated by aggravating factors for limited periods of time (hours, days, weeks), and resolves when risk factors are effectively targeted coping/problem-solving skills, etc.)
Rudd, M.D. (2006). Fluid vulnerability theory: a cognitive approach to understanding the process of acute and chronic risk. In T.E. Ellis (Ed.), Cognition and Suicide: Theory, Research, and Therapy. Washington, DC: American Psychological Association.
|
Acute Suicide Risk Continuum
|
Risk Level
|
Description
|
|
Mild
|
Suicidal ideation of limited frequency, intensity, duration, and specificity. Morbid ideations may be present. There are no identifiable plans; no associated intent, mild dysphoria, and related symptoms; good self-control; few other risk factors; and the presence of identifiable protective factors, including social support.
|
|
Moderate
|
Frequent suicidal ideation with limited intensity and duration, some specificity in terms of plans, no intent, good self-control, limited dysphoria and other symptoms, some risk and protective factors, including social support.
|
|
High
|
Frequent, intense, and enduring suicidal ideation; specific plans; some objective markers of intent (e.g., lethal and available method choice, some preparatory behavior); subjective intent may or may not be present; some impairment in self-control; severe dysphoria and/or other symptoms; multiple risk factors present; and few protective factors, particularly social support.
|
|
Protective Factors for Suicide
Protective factors reduce the likelihood of suicide; they enhance resilience and may serve to counterbalance risk factors.
- Effective clinical care for mental, physical, and substance use disorders
- Easy access to a variety of clinical interventions and support for help-seeking
- Restricted access to highly lethal means of suicide
- Strong connections to family and community support
- Support through ongoing medical and mental health care relationships
- Skills in problem solving, conflict resolution and nonviolent handling of disputes
- Cultural and religious beliefs that discourage suicide and support self-preservation.
Youth-Specific Protective Factors
- Contact with a caring adult
- Sense of connection or participation in school
- Positive self-esteem and coping skills
- Access to and care for mental/physical/substance disorders
|
Recommended Response Protocol Based on Risk Level
|
Risk Level
|
Indicated Response
|
|
FOR ALL CLIENTS
|
Complete a Safety Plan and Commitment to Treatment Statement, incorporating a crisis response plan regardless of risk level. This should be a part of the informed consent process for each and every client. Also, have the client sign the necessary release of information forms to allow for input from selected family members.
|
|
Mild
|
No particular changes in ongoing treatment. Evaluation of any expressed suicidal ideation to monitor change in risk is needed on an ongoing basis.
|
|
Moderate
|
1. Recurrent evaluation of need for hospitalization.
2. Increase in frequency or duration of outpatient visits.
3. Active involvement of the family.
4. Frequent reevaluation of treatment plan goals.
5. 24-hour availability of emergency or crisis services for patient.
6. Frequent reevaluation of suicide risk, noting specific changes that reduce or elevate risk.
7. Consideration of medication if symptoms worsen or persist.
8. Use of telephone contacts for monitoring.
9. Frequent input from family members with respect to indicators.
10. Professional consultation as indicated.
|
|
High
|
Immediate evaluation for inpatient hospitalization (voluntary or involuntary, depending on
situation). In cases of extreme risk, the only appropriate response is hospitalization for stabilization.
|
|
Develop a Safety Plan on Initial Engagement with Suicidal Client
Instructions for Developing a Safety Plan
Step 1: Recognizing Warning Signs
1. Ask: “How will you know when the safety plan should be used?”
2. Ask: “What do you experience when you start to think about suicide or feel extremely distressed?”
List warning signs (thoughts, images, thinking processes, mood, and/or behaviors) using the Clients’ own words.
Step 2: Using Internal Coping Strategies
1. Ask: “What can you do, on your own, if you become suicidal again, to help yourself not to act on your thoughts or urges?”
2. Ask: “How likely do you think you would be able to do this step during a time of crisis?”
If doubt about using coping strategies is expressed
3. Ask: “What might stand in the way of you thinking of these activities or doing them if you think of them?”
Use a collaborative, problem solving approach to ensure that potential roadblocks are addressed and/or that alternative coping strategies are identified.
Step 3: Social Contacts Who May Distract from the Crisis
- ____________________________
- ____________________________
- ____________________________
- ____________________________
- ____________________________
Instruct client to use Step 3 if Step 2 does not resolve the crisis or lower risk.
1. Ask: “Who or what social settings help you take your mind off your problems at least for a little while? “Who helps you feel better when you socialize with them?”
2. Ask Client to list several people and social settings, in case the first option is unavailable.
3. Ask for safe places the client can go to do be around people, e.g. coffee shop.
Remember, in this step, suicidal thoughts and feelings are not revealed.
Step 4: Contacting Family Members or Friends Who May Offer Help to Resolve a Crisis
- ____________________________
- ____________________________
- ____________________________
- ____________________________
- ____________________________
Instruct client to use Step 4 if Step 3 does not resolve the crisis or lower risk.
Ask: “Among your family or friends, who do you think you could contact for help during a crisis?” or “Who is supportive of you and who do you feel that you can talk with when you’re under stress?”
Ask client to list several people, in case they cannot reach the first person on the list. Prioritize the list. In this step, unlike the previous step, patients reveal they are in crisis.
Ask: “How likely would you be willing to contact these individuals?”
If doubt is expressed about contacting individuals, identify potential obstacles and problem solve ways to overcome them.
Step 5: Contacting Professionals and Agencies
- ____________________________
- ____________________________
- ____________________________
- ____________________________
- ____________________________
Instruct client to use Step 5 if Step 4 does not resolve the crisis or lower risk.
Ask: “Who are the mental health professionals that we should identify to be on your safety plan?” and “Are there other health care providers?”
List names, numbers and/or locations of clinicians, local urgent care services, Suicide Prevention Hotlines
If doubt is expressed about contacting individuals, identify potential obstacles and problem solve ways to overcome them.
Step 6: Reducing the Potential for Use of Lethal Means
- ____________________________
- ____________________________
- ____________________________
- ____________________________
- ____________________________
The counselor should ask client which means would be considered to be used during a suicidal crisis and collaboratively identify ways to secure or limit access to these means.
For methods with low lethality, counselor may ask client to remove or restrict access to these methods on his/her own.
Restricting the client’s access to a highly lethal method should be done by a designated, responsible person—usually a family member or close friend, or the police.
|
Develop a Safety Plan
Purpose: Counselor and client complete a Safety Plan together, and client keeps it for future reference as needed. Here is an example of a Safety Plan:
|
My Personal Safety Plan
When I need to talk about how I’m feeling, I will contact my social supports:
Names of Friends(s)
Names of Family member(s)
Emergency Contacts:
Friends and/or Family: Names and Telephone #
Professional(s): Name(s) and Telephone #
If I still feel suicidal and out-of-control, I will go to the nearest hospital emergency department or call 911:
What might keep me from implementing this Safety Plan?
Who will I share this plan with?
Where will I keep this plan?
In order to keep myself safe, I will remove or safely store things I could use to hurt myself:
Firearms:
Medications:
Household poisons:
Sharp or other dangerous objects:
I can sometimes anticipate when I need to take extra care of myself. These are the people, places and situations that trigger the most stress for me:
1.
2.
3.
These are my warning signs that things are starting to get out of control:
Thoughts:
Feelings:
Behaviors:
Symptoms:
My most effective coping strategies:
These things work to help calm me or change my thoughts:
These are healthy activities I can use to distract myself:
|
Note: Once the client and therapist have finished the Safety Plan, the Therapist also can give the client a handout called Overcomng Suicidal Thoughts and Feelings available at:
|
Client Commitment to Treatment Statement
At the end of the initial session with the client make sure that the client signs a Committment to Treatment contract. The intent is to inform the client that the counselor will take steps if the client does not communicate with or show up for appointments with the counselor. It also commits the client work on the Safety Plan and the treatment program outlined in the initial session.
|
Commitment to Treatment Statement
I, ______________________, agree to make a commitment to the treatment process. I understand that this means I have agreed to be actively involved in all aspects of treatment, including:
1. Attending appointments (or letting my counselor know when I can’t make it);
2. Setting goals;
3. Voicing my opinions, thoughts, and feelings honestly and openly with my counselor (whether they are negative or positive, but most importantly my negative feelings);
4. Being actively involved during appointments;
5. Completing homework assignments;
6. Taking my medications as prescribed;
7. Experimenting with new behaviors and new ways of doing things;
8. Implementing my crisis response plan when needed;
9. Any additional terms that my counselor and I agree to:
I understand and acknowledge that, to a large degree, a successful treatment outcome depends on the amount of energy and effort I make. If I feel like treatment is not working. I agree to discuss it with my counselor and attempt to come to a common understanding as to what the problems are and identify potential solutions.
I also understand and acknowledge that if I do not show up for an appointment without notifying my counselor, my counselor might contact individuals within my social support network, in order to confirm my safety.
In short, I agree to make a commitment to treatment, and a commitment to living.
This agreement will apply for the duration of our treatment plan, which will be reviewed and modified on the following date: ________________.
Client signature: ___________________________________ Date: ________________
Counselor signature: ________________________________ Date: _______________
|
|
Removal of Means for Suicide
At the time of the initial engagement with the client is important if the client has a means for suicide at home that it be removed and secured with a trustworthy person who will not return the means to the client unless approved by the counselor. Such a form would include the following information:
Means Receipt
Questions? Contact your provider: _____________________________________________
Emergencies call: 911
|
Client Name
|
|
|
Securer
|
|
|
Address
|
|
|
Email
|
|
|
Work Phone
|
|
|
Cell Phone
|
|
|
Type of means
|
|
|
Safety Measures
|
Removed (Describe: ______________________)
Secured (Describe: _______________________)
|
|
Release Terms
|
To be released to client upon notification by counselor
|
Thank you for your cooperation!
|
Reduce Emotional Vulnerability: ABC’s
A: Accumulate Positive Experiences
In the Short Term:
Do pleasant things that are possible right now.
Increase pleasant activities that lead to positive emotions.
Do one thing each day from the Pleasant Activities List which have been brainstormed
In the Long Term:
Make changes in your life so positive events will occur more often.
Build a life worth living.
Work towards goals:
Make list of positive events you want.
List small steps towards goals.
Take first step.
Pay attention to relationships:
Repair old relationships.
Reach out for new relationships.
Work on current relationships.
Avoid avoiding
Avoid giving up
B: Build Mastery
Schedule one or more activities each day to build a sense of accomplishment
C: Cope Ahead
Create a plan ahead of time so that you are prepared to cope skillfully with emotional situations. Imagine yourself coping effectively.
|
Build Resilience
What is Resilience?
Everyone experiences stress and difficult circumstances during their life.
Most people can handle these tough times and may even be able to make something good from a difficult situation.
Resilience is the ability to bounce back after experiencing trauma or stress, to adapt to changing circumstances and respond positively to difficult situations.
It is the ability to learn and grow through the positive and the negative experiences of life, turning potentially traumatic experiences into constructive ones.
Being resilient involves engaging with friends and family for support, and using coping strategies and problem-solving skills effectively to work through difficulties.
Factors That Contribute to Individual Well-Being
1. Self Image: sense of self, including self-esteem secure identity, ability to cope, and mental health and well-being
2. Behavior: social skills including life skills, communication, flexibility, and caring
3. Spirit: sense of purpose, including motivation, purpose in life, spirituality, beliefs, and meaning
4. Heart: emotional stability, including emotional skills, humor, and empathy
5. Mind: problem solving skills, including planning, problem-solving, help-seeking, and critical and creative-thinking.
6. Body: physical health, physical energy, and physical capacity
The Four Main Factors That Influence A Person’s Reaction to Life Events
1. Individual Health and Well-Being
Sense of self, social skills, sense of purpose, emotional stability, problem-solving skills, and physical health.
2. Pre-Disposing or Individual Factors
Genes, gender and gender identity, personality, ethnicity/culture, socio-economic background, and social/geographic inclusion or isolation. 3. Life History and Experience
Family history and context, previous physical and mental health, exposure to trauma, past social and cultural experiences, and history of coping.
4. Social and Community Support
Support and understanding from family, friends, local doctor, local community, school, level of connectedness, safe and secure support environments, and availability of sensitive professionals/carers and mental health practitioners.
How to Increase Personal Resiliency
1. Look after relationships: Family and close friends are usually willing to listen, provide support and often have helpful ideas or know where to go for help in all sort of situations.
2. Think well of yourself: Identify what you are good at, and what you need to learn, to help you face the future. Invest time and energy in developing new skills.
3. Practice helpful ways of thinking: Challenge negative thoughts and look for alternative solutions to problems, to find optimistic ways of viewing any situation.
4. Maintain health: Look after your physical health. Poor diet and lack of exercise may contribute to negative thinking.
5. Develop a sense of connectedness: Get involved in enjoyable community activities such as social or sporting activities or volunteering; it will help broaden social networks and counter feelings of isolation.
6. Don’t tackle major problems alone: Ask for help and support when you need it. Don’t be afraid of expressing your emotions and offer assistance in turn to those around you.
How to Build Community Resilience
1. Build community cohesion: Communities that work together and work towards common goals have a greater sense of optimism and morale.
2. Build stronger families: Community education programs can be helpful in improving skills in areas such as parenting, communication, relationships, money management, stress management and coping skills.
3. Develop cultural competency: Communities that value their cultural diversity can work more strongly together when times are hard. Education and training in cultural competency for key community members help to ensure that the right support is available to everyone when they need it.
4. Build safe and healthy environments including lowering the threat of violence: Communities that are safe and secure are more likely to manage difficult circumstances positively.
5. Encourage healthy lifestyles: Promote regular exercise in the community by providing education and awareness programs and access to bike or walking paths, parks, and other sport/community facilities.
|
Cultural Competence
Cultural competence is the process of communicating with people from diverse geographic, ethnic, racial, and cultural, economic, and social backgrounds. Becoming culturally competent requires knowledge and skill development at policymaking, administration, and practice.
Steps to Take to Grow in Cultural Competence
1. Become more aware of the various cultures that exist within your community.
2. Assess personal cultural values while acknowledging each of our own perceptions of the world
3. Work to understand the dynamics that may occur when members of different cultures interact
Culturally Appropriate Strategies
1. Prevention strategies are culturally competent when they demonstrate sensitivity to cultural differences and similarities, while demonstrating effectiveness in using cultural symbols to communicate a message.
2. Seek input from your target population before developing and implementing prevention strategies.
3. Develop written guidelines that help guide the cultural competence of program staff.
4. Continuously review all strategies, policies, procedures, and practices to ensure they are culturally competent
The Importance of Faith/Spirituality
Reason for living? Suicide is not an option:
In examining the relationship between spirituality, social desirability, and reasons for living, a positive correlation was found between religious well-being and the total reason for living.
Suicide unacceptable:
There is a strong relationship between the adaptive cognitive beliefs which people report as reasons for not considering suicide and their existential beliefs. People with attributes of higher education, lower religiosity, and high commitment to freedom of expression were more likely to consider suicide as acceptable.
Suicidal ideation:
In a study on the relationship between religion and suicidal ideation in a cohort of Latin-American immigrants, it was found that self-perception of religiosity, influence of religion, and church attendance were significantly negatively associated with suicidal ideation. An analysis showed that the influence of religion was a significant predictor of suicidal ideation.
Suicide attempts: In a study examining the personal factors associated with suicidal behavior among African American women and men, found that, compared with non-attempters, attempters reported more psychological distress, aggression, substance use, maladaptive coping strategies, less religiosity/spirituality, and lower levels of ethnic identity.
|
|
|