In Cognitive Behavior Therapy, Crisis Intervention
1. Helps client recognize crisis trigger and help client understand thoughts/ feelings about the trigger
2. Help client act in a way that will deactivate suicidal thoughts
3. Help client gain access to emergency care if the suggested strategies are ineffective
Initial Management Post-Suicide Risk Assessment
Match care level to risk level
Secure client’s safety
1. Psychoeducation for client
2. Limit access to means
3. Complete a thorough safety plan
4. Address needs/increase social support
5. Increase coping skills
Crisis Intervention: Safety Planning
Developed collaboratively with client
1. Mood regulation techniques
2. Pleasant activities
3. Emergency numbers
Six Steps in Safety Planning
Step 1: Warning Signs
Step 2: Internal Coping Strategies
Step 3: Distractions
Step 4: Family/Friends
Step 5: Emergency contacts
Step 6: Safe Environment
Implementation of a Safety Plan
1. Review each step and obtain feedback
2. Estimate the likelihood of following through (0-100%)
3. Specify location of safety plan
4. Revise at subsequent meetings as new skills are learned or as the social network is expanded
(Stanley & Brown, 2008); (Wenzel at al., 2009)
Promising Means Restriction Intervention
1. Means Restriction–Actual process of limiting/removing access to lethal
means
2. Means Restriction Counseling–Educating client and supportive others about risk
associated with easy availability of means
3. Collaboratively work with client and support person to limit/remove access to means until the suicidal risk has lessened
Means Restriction Counseling
1. Describe rationale for means restriction: emphasis on ensuring safety and overcoming suicidality
2. Conduct means restriction counseling: a collaborative plan of how means for suicide will be restricted
3. Implementation of means restriction: The enactment of the agreed-upon measures from the Means Restriction Agreement
a. Means receipt (client and significant other)
b. Crisis support plan (significant other)
(Rudd & Bryan (2011); (Bryan et al., 2011); (Rudd et al., 2015)
Means Restriction Counseling: Watch this Video to see how Means Restriction Counseling proceeds:
https://www.youtube.com/watch?v=FUtdOrmFr38&feature=youtu.be
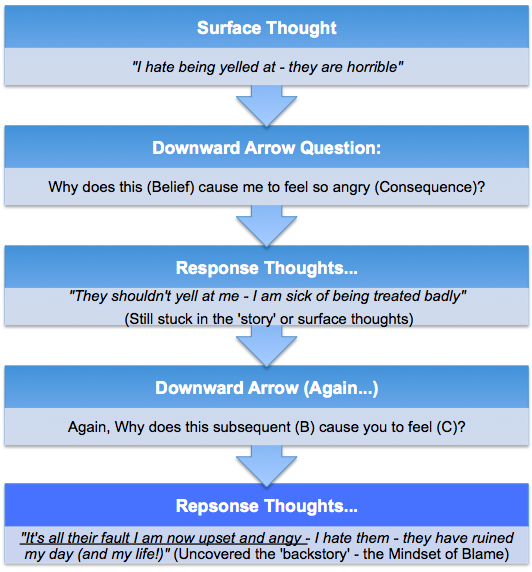
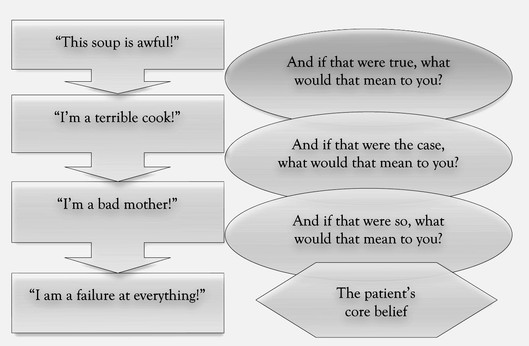
Constructing a Timeline of the Suicidal Crisis
Incorporates…
1. Activating Event
2. Cognitions
• Key automatic thoughts
• Dysfunctional assumptions
• Core beliefs
3. Emotions
4. Behavioral Responses
(Wenzel et al., 2009)
Assists in…
1. Developing a cognitive case conceptualization
2. Identifying points for intervention
3. Preparing for the relapse prevention protocol
(Wenzel et al., 2009)
Treatment Planning
Purpose: To determine skills deficits which need improvement and dysfunctional beliefs to be modified
1. Developing Treatment Goals
2. Selecting an Intervention Strategy
3. Prevention of future suicidal behavior–Client may be reluctant to establish this as a treatment goal
4. Addressing dispositional vulnerability factors
5. Secondary goals –Approach these in context of recent suicide crises and risk for future suicidal behavior
6. Modifying core beliefs
(Wenzel et al., 2009)
Cognitive Case Conceptualization
Goal: To develop a more in-depth understanding of the suicidal crisis
1. Identify: Early experiences, core beliefs, Intermediate beliefs, key automatic thoughts
2. Identify dispositional vulnerability factors which have the potential to…
- Activate suicide-relevant schemas
- Exacerbate suicidal crises
3. Identify suicide-relevant cognitive processes
(Wenzel et al., 2009)