Steps to Take to Avoid Compassion Fatigue
|
Professional Mental Health Ethics
A Training Resource
By James J Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
Steps to Take to Avoid Compassion Fatigue
CEU's: 3 hours based on request (CE Broker Tracking #: 20-615488)
Resource for Course on Coping.us: http://www.coping.us/professionalmentalhealthethics/avoidcompassionfatigue.html
Description of Program: Professional Helpers are prone to Compassion Fatigue or Burnout on the job. Compassion fatigue is thought to be a combination of secondary traumatization and burnout precipitated by the care delivery that brings professional helpers into contact with the suffering of their helpees. Compassion fatigue is when helpers have such deep empathy they develop symptoms of trauma like their helpees. Compassion Fatigue can also resemble burnout which occurs when emotional exhaustion is experienced due to increased workload and institutional stress and does not involve trauma. Compassion Fatigue can have detrimental effects on clinical relationships since helpers suffering from it often either grow distant from their helpees or get too close to them. Professional Helpers need to learn how to improve their self-care, handle the stressors involved in their work by self-care activities such as Mindfulness Meditation, Yoga, Exercise, Good Diet, Healthy Sleep. Etc.
Learning Objectives
1. To learn how to identify if helpers are having problems maintaining a healthy focus with their helpees.
2, To learn how to identify if helpers are a compulsive fixers or rescuers which could impact their maintaining healthy working relationships with their helpees.
3. To learn how to assist helpers if they are suffering from Compassion Fatigue which could impact their maintaining healthy working relationships with their helpees.
4, To identify tips on how helpers can maintain healthy working relationships with their helpees while maintaining their own emotional and physical health.
|
|
Introduction to Compassion Fatigue
In this video Patricia Smith identifies:
"Compassion Fatigue is a state experienced by those helping people or animals in distress; it is an extreme state of tension and preoccupation with the suffering of those being helped to the degree that it can create a secondary traumatic stress for the helper."
Dr. Charles Figley
Professor, Paul Henry Kurzweg Distinguished Chair
Director, Tulane Traumatology Institute
Tulane University, New Orleans, LA
Caring too much can hurt. When caregivers focus on others without practicing self-care, destructive behaviors can surface. Apathy, isolation, bottled up emotions and substance abuse head a long list of symptoms associated with the secondary traumatic stress disorder now labeled: Compassion Fatigue
While the effects of Compassion Fatigue can cause pain and suffering, learning to recognize and manage its symptoms is the first step toward healing. The Compassion Fatigue Awareness Project© is dedicated to educating caregivers about authentic, sustainable self-care and aiding organizations in their goal of providing healthy, compassionate care to those whom they serve.
|
Goals of this Online Program
1.Identify Compassion Fatigue through Self-Assessment & Remediation Plan for Health care Helpers
2.Identify Physical exercises, aerobic & mobility activities that improve self-care for Health care Helpers
3.Identify a Nutritional regimen that sustains health, energy & cognitive clarity of health care Helpers
4.Identify how competency based continuing education improves the self-care of Health care Helpers
5.Identify how to maintain one’s sense of humor & emotional balance as a Health care Helpers
6.Identify what you are willing to commit to which will improve your self-care from this point on
|
Background on Compassion Fatigue
Clinicians who work with people in a variety of settings are confronted with a new workplace epidemic which is known as Compassion Fatigue. The family members and clinicians who are most susceptible to this condition work with people who fit one or more of the following categories:
- Survivors of torture, trauma, or natural or man-made disasters
- Survivors of Physical, Sexual and Emotional Abuse
-
Injured veterans survivors of the Afghanistan and Iraq Wars or other prior wars
-
Veterans suffering from PTSD from being in the Afghanistan and Iraq Wars or other prior wars
-
Patients dealing with life threatening illness like cancer, heart and lung conditions, HIV-AIDS, or other systemic health conditions
-
Hospice eligible individuals facing imminent death due to old age, injury, disease or illnesses
Compassion fatigue is thought to be a combination of secondary traumatization and burnout precipitated by the care delivery that brings health-care professionals into contact with the suffering (Szabo, 2006).
|
"Compassion fatigue is when caregivers have such deep empathy they develop symptoms of trauma similar to the patient” according to director of the Army Institute of Surgical Research Colonel Kathryn Gaylord (Wilson, 2008). Wilson points out that Compassion Fatigue can also resemble burn out which occurs when emotional exhaustion is experienced due to increased workload and institutional stress and does not involve trauma (2008). Wilson finally points out that Compassion Fatigue can have detrimental effects on doctor patient relationships since doctors suffering from the disorder often either grow distant from patients or get too close (2008).
It is believed that Secondary Traumatic Stress might be a contributing factor to developing Compassion Fatigue. According to Bride (2007) it is when clinicians who come into continued, close contact with trauma survivors may also experience emotional disruption, becoming indirect victims of the trauma. These clinicians Bride (2007) explains have the natural, consequent behaviors and emotions resulting from knowledge about a traumatizing event experienced by the trauma survivors they come in contact with resulting in them experiencing a secondary stress from helping or wanting to help these traumatized or suffering people.
|
The opposite of Compassion Fatigue is Compassion Satisfaction, which is the ability for clinicians to derive a great sense of meaning and purpose from their work (Tyson, 2007). Tyson goes on to say that Compassion Satisfaction may aid in alleviating existential terror endemic to the human condition when a society is at war since it may be an important buffer in managing and transcending alterations in belief systems, and physiological or emotional reactions seen in Compassion Fatigue (2007).
Charles Figley (1995) in his ground breaking work on Compassion Fatigue postulated that there were four reasons why clinicians and family members would develop this condition. They were:
-
Poor self-care
-
Previous unresolved trauma
-
Inability or refusal to control work stressors
-
Lack of satisfaction for the work
Abendroth and Flannery (2006) identified the following four variables as being predictors if Hospice Nurses were more likely to experience Compassion Fatigue. They were:
It is imperative that clinicians and family members focus on preventing or dealing with Compassion Fatigue according to Linley and Joseph (2007) because they need to take steps to ensure that they are functioning at their best in the therapeutic relationship with the people they serve and live with through facilitating their own personal well–being and avoiding burnout.
|
Compassion Fatigue Self-Assessment
Take some time now to do your own self-assessment to see if you are suffering from signs or symptoms of Compassion Fatigue.
Directions: Rate each item on a scale of 1-10 for each of the following items as it applies to you at this time in your life.
|
1 5 10
never experience...occasionally experience...frequently experience
|
|
-
Overstressed, muscle tightness, having difficulty sleeping
-
Feeling of being “under supported,” sensing that others are “uncaring”
-
A sense of being lackadaisical
-
Chronic feeling of “being sick,” overtired, or having general fatigue
-
State of being worried: “having concerns on my mind”
-
Asking “Why do I stay here?”
-
Feelings of guilt
-
Disillusionment on the job or with home life
-
Feelings of being “let down”
-
Speaking of work or home as if I am not the “real me” when there
-
Feelings of helplessness like a victim
-
Desire to be allowed to be the “real me” at home or on the job
-
Feeling that too many expectations are heaped on me
-
Blaming others for everything
-
Lack of caring for family, co-workers, others
-
Feelings of self-righteousness
-
Feeling and acting very defensively
-
Maintaining an unapproachable attitude
-
Questioning personal values and judgments
-
Feeling intimidated by people
-
Asking “Is this all there is?”
-
Lack of interest in the outside world
-
Cutting self, off from family and/or friends
-
Feeling like “I am working harder but experiencing fewer successes”
-
Feeling unappreciated
-
Escaping into increased workload
-
Desiring to run away
-
Continuous state of depression, feeling down or blue
-
Not willing to take time for a vacation because “I’ve got to work”
-
Frustration with the system
-
Feelings of paranoia
-
Not looking forward to coming to work in the morning
-
Daydreaming or fantasizing during the day
-
Sense of failure in everything I try
-
Tendency to catch more minor illnesses and staying sick longer
-
Withdrawal from important relationships
|
Interpretation of your Self-Assessment
If you rated three or more items over 8 or if you rated 5-10 over 5, you are most likely experiencing some level of compassion fatigue and it would be important for you to take action to prevent it from getting worse or happening at all in the first place.
|
|
What Level of Stress Do You Have in Your Personal Life?
Personal life events analysis:To learn the level of stress (distress) in your life, mark down in your journal the value at the right of each of the following events if it has occurred within the past 12 -24 months:
Event (Value)
-
Death of spouse (100)
-
Divorce (73)
-
Marital separation (65)
-
Jail term (63)
-
Death of close family member (63)
-
Personal injury or illness (53)
-
Marriage (50)
-
Fired from job (47)
-
Marital reconciliation (45)
-
Retirement (45)
-
Change in family member's health (44)
-
Pregnancy (40)
-
Sexual difficulties (39)
-
Addition to family (39)
-
Business readjustment (39)
-
Change in financial status (38)
-
Death of close friend (37)
-
Career change (36)
-
Change in number of marital arguments (35)
-
Mortgage or loan over $10,000 (31)
-
Foreclosure of mortgage or loan (30)
-
Change in work responsibilities (29)
-
Son or daughter leaving home (29)
-
Trouble with in-laws (29)
-
Outstanding personal achievement (28)
-
Spouse begins or ceases working (26)
-
Starting or finishing school (26)
-
Change in living conditions (25)
-
Revision of personal habits (24)
-
Trouble with boss (23)
-
Change in work hours, conditions (20)
-
Change in residence (20)
-
Change in schools (20)
-
Change in recreational habits (19)
-
Change in church activities (19)
-
Change in social activities (18)
-
Mortgage or loan under $10,000 (17)
-
Change in sleeping habits (16)
-
Change in number of family gatherings (15)
-
Change in eating habits (15)
-
Vacation (13)
-
Christmas season (12)
-
Minor violation of the law (11)
How to analyze your score:
Add the values of all the items you identified with. If your total score is more than 150, find ways to reduce stress in your daily life so that your stress level doesn't increase. The higher the score, the harder one needs to work at staying physically well.
|
Suggested uses for personal life-events analysis:
-
Become familiar with the different events and the amounts of stress they promote.
-
Put the list of events where your family can easily refer to it several times a day.
-
Practice recognizing the stress level when one of these events happens.
-
Think about the meaning of the event for you and identify your feelings.
-
Think about the different ways you can adjust to the event.
-
Take your time in arriving at decisions.
-
Anticipate life changes and plan for them well in advance whenever possible.
-
Pace yourself. It can be done even if you are in a hurry.
-
Look at the accomplishment of a task as a part of ongoing daily living; avoid looking at such an achievement as a stopping point. Congratulate yourself and push ahead.
-
Recognize that your internal mechanism of coping with stress is directly tied to how your health and well-being will be influenced by it.
|
|
Are you a Compulsive Fixer-Rescuer?
Directions: Read the following statements to figure out if you are a Compulsive Fixer and or Rescuer? On a scale of 1 to 10 rate how true this item is for you. Use this scale:
1 = not at all true for me 5 = sometimes true for me 10 = always true for me
|
1. Do you want to help your clients and or their families to handle situations they find themselves in even when the clients or their families have not asked for your help?
2. Do you find that you really are trying to “fix” the lives of your clients and or their families when in fact there are many things in their lives which cannot be fixed and therefore you hit dead ends in your attempts to “fix” their unsolvable problems?
3. Do you find it hard not to “butt in” and offer your “two cents” in almost every situation your clients and or their families open up to tell you about?
4. Do you bristle or resent it when given feedback on your helping skills especially if the feedback is concerned about you possibly “burning out” due to your overextending yourself into the lives of your clients and or their families?
5. Have you ever questioned yourself as to why it is that you spend more time in your life in helping your clients and or their families achieve the things they need in their lives and yet you ignore and spend little time in meeting your own life needs?
6. Do you find that you are always ready with an answer or solution for anyone you come upon who is in major need even when the solutions are close to impossible to achieve given the dire nature of the clients’ and or their families’ needs?
7. Do you find yourself currently compulsively driven behavior to rescue or help your clients and their families to be the way you believe they should be?
8. Do you find yourself seeing your clients and or their families as in need and find your automatic response pattern to this reality it to fix it and make it better?
9. Do you believe that, unless everything is just right for your clients and or their families that then can never fully be happy in life?
10. Do you find yourself developing into an obsessive need to have everything in your clients and or their families’ lives to be perfect or correct in order for you to be comfortable enough to be relaxed and accepting of circumstances?
11. Do you find yourself having an inability to accept your clients and or their families the way they are and then chronically attempting at changing them even if they are unchangeable?
12. Do you find yourself acting on the belief that you have more knowledge than your clients and or their families as to what is good for them so you strive to correct their thinking to see the light in your way?
13. Do you find yourself having an inability to maintain emotional detachment from the circumstances in your clients and or their families’ lives that are hurting or troublesome to witness so that you proceed to fix them even if this means that they are hindered from personal growth and accepting personal responsibility for their own actions?
14. Do you have an inability to not give advice, suggestions, or make offers of help, even when you know in doing so that it will hinder your clients and or their families’ growth and personal mastery in life?
15. Do you find yourself interfering in business and personal affairs to help your client clients and or their families even when they haven't asked for your help or assistance?
16. Do you find yourself driven to feel needed or wanted which leads you to become overly involved and overresponsible in your relationships with your clients and or their families?
17. Do you see that you are caught up in a pattern of needing to get approval and recognition from your clients and or their families for helping with the belief that this is the only way you can have meaning in life?
|
Results: if you have answered 5 more items with scores of 5 or higher there is a strong possibility that you are maintaining weak boundaries with your clients and or their families due to being a compulsive fixer or rescuer.
|
|
Results of EMPATH Self-Assessment
SCORE OF 0 - 25: You have some Empath traits, but wouldn't be considered a true Empath. It's important to make sure that you still take care of yourself and don't let yourself get overwhelmed, but it's likely you are pretty balanced between helping others and setting good boundaries.
SCORE OF 25 - 50: This score on the Empath Test shows that you are definitely an Empath. You sense things in a way that's different from the average person. You aren't just relating to someone's feelings, you are sensing them as your own. You likely get exhausted sometimes and wonder why, without realizing you are giving out too much positive energy and taking in too much negative energy from around you. While you are fairly balanced if you are in this range, there's no doubt you'd benefit from tools and resources to help you to use your EFP (extra-feeling perception) to be a benefit to yourself and the world.
SCORE OF 50 – 75: You are an "extreme Empath.". You have the ability to soak in others' emotions without consciously knowing you are doing so. You sense the "vibe" of a room or place without visual clues (such as tears, yelling, or slamming of doors). More importantly, if you are scoring this high on the Empath Test, then you are extremely open to the pain and suffering of the world, and you likely get overwhelmed by trying to do too much or help too many people at once. If you don't get some tools and resources to help you, these extreme Empath traits can cause you to get very sick (chronic fatigue is extremely common among Empaths who score like this and don't have the tools to take care of themselves).
SOURCE: http://www.tarameyerrobson.com/empath-test/
|
Professional Quality of Life Scale (PROQOL)
The PROQOL Self-Assessment will provide for Helpers three measures:
- Compassion Satisfaction
- Burnout
- Secondary Traumatic Stress
When Helpers help people they have direct contact with their lives. As many helpers have found, their compassion for those they help can affect them in positive and negative ways. On the PROQOL are some questions about these experiences, both positive and negative, as a helper. When taking this self-assessment, consider each of the questions about you as a helper and your current work situation. Select the number that honestly reflects how frequently you experienced these things in the last 30 days.
|
Explanation of the Three Variable Measured on the PROQOL
1. Compassion Satisfaction
Compassion satisfaction is about the pleasure helpers derive from being able to do their work well. For example, they may feel like it is a pleasure to help others through their work. They may feel positively about their colleagues or their ability to contribute to the work setting or even the greater good of society. Higher scores on this scale represent a greater satisfaction related to their ability to be an effective caregiver in their job.
The average score is 50 (SD 10; alpha scale reliability .88). About 25% of people score higher than 57 and about 25% of people score below 43. If you are in the higher range, you probably derive a good deal of professional satisfaction from your position. If your scores are below 40, you may either find problems with your job, or there may be some other reason—for example, you might derive your satisfaction from activities other than your job.
|
2. Burnout
Most people have an intuitive idea of what burnout is. From the research perspective, burnout is one of the elements of Compassion Fatigue (CF). It is associated with feelings of hopelessness and difficulties in dealing with work or in doing your job effectively. These negative feelings usually have a gradual onset. They can reflect the feeling that your efforts make no difference, or they can be associated with a very high workload or a non-supportive work environment. Higher scores on this scale mean that you are at higher risk for burnout.
The average score on the burnout scale is 50 (SD 10; alpha scale reliability .75). About 25% of people score above 57 and about 25% of people score below 43. If your score is below 43, this probably reflects positive feelings about your ability to be effective in your work. If you score above 57 you may wish to think about what at work makes you feel like you are not effective in your position. Your score may reflect your mood; perhaps you were having a “bad day” or are in need of some time off. If the high score persists or if it is reflective of other worries, it may be a cause for concern.
|
3. Secondary Traumatic Stress
The second component of Compassion Fatigue (CF) is secondary traumatic stress (STS). It is about Helpers' work related, secondary exposure to extremely or traumatically stressful events. Developing problems due to exposure to other’s trauma is somewhat rare but does happen to many people who care for those who have experienced extremely or traumatically stressful events. For example, Helpers may repeatedly hear stories about the traumatic things that happen to other people, commonly called Vicarious Traumatization. If their work puts them directly in the path of danger, for example, field work in a war or area of civil violence, this is not secondary exposure; their exposure is primary. However, if they are exposed to others’ traumatic events as a result of their work, for example, as a therapist or an emergency worker, this is secondary exposure. The symptoms of STS are usually rapid in onset and associated with a particular event. They may include being afraid, having difficulty sleeping, having images of the upsetting event pop into mind, or avoiding things that remind them of the event.
The average score on this scale is 50 (SD 10; alpha scale reliability .81). About 25% of people score below 43 and about 25% of people score above 57. If your score is above 57, you may want to take some time to think about what at work may be frightening to you or if there is some other reason for the elevated score. While higher scores do not mean that you do have a problem, they are an indication that you may want to examine how you feel about your work and your work environment. You may wish to discuss this with your supervisor, a colleague, or a health care professional.
B. Hudnall Stamm, 2009-2012. Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL). www.proqol.org..
|
What can be done in the Helpers Work Place to Lessen the Impact of Compassion Fatigue?
It is imperative that fsupervisors and administrators work to establish a Compassion Fatigue prevention program in their families and departments or agencies including some of these best practices:
- Identify realistic attainable goals r for each department and evaluate accordingly
- Help staff to maintain personal growth both at home and on the job
- Encourage staff to develop an active outside life with a variety of interests
- Encourage staff to personalize the family or work environment with meaningful pictures, objects, colors, etc.
- Encourage staff to be comfortable with themselves by setting limits how far to become involved with clients and colleagues
- Encourage and practice good communication skills on the job
- Provide for flexible living or working conditions on the job
- Encourage trying new ideas “outside of the box”
- Sponsor “decompression techniques” activities such as meditation or exercise that relieve tension and put staff into a more relaxed state
- Build support systems among staff to discuss problems and help each other look for solutions. Don't just air gripes - look for solutions
|
What Can You Do to Address Compassion Fatigue?
You can do any or all of the following best practices:
To back up this self-help plan, Radey and Figley (2007) point out Helpers need to do the following four self-care steps to avoid suffering from Compassion Fatigue:
If Helpers are able to achieve all four of these preventive tasks, they assure that they will thrive as compassionate professionals.
|
Politsky (2007) reported on a Compassion Fatigue Prevention program implemented in her Oncology Department. This program offered staff a safe place, among colleagues to discuss their recent feelings and de-stress. Participants were provided services such as yoga, meditation and therapeutic massage. All staff completed a Compassion Fatigue Survey and all staff were treated with a 45 minute therapeutic massage. A program does not need to necessarily utilize all of these components but it is important to begin to do something now to insure that staff are being protected and assisted to address this problem.
At the minimum it is important for clinical program departments to run training on the Compassion Fatigue and encourage self-assessment and monitoring for it. Sprang, Clark and Whitt-Woosley (2007) found that specialized trauma training did enhance Compassion Satisfaction and reduced levels of Compassion Fatigue and Burnout, suggesting that knowledge and training might provide some protection against the deleterious effects of trauma exposure.
Dealing with Compassion Fatigue is a TEAM effort which requires all the administration on the job, co-workers on the job and significant others to understand that it takes a lot of effort to prevent and deal with this insidious and disabling condition!
|
|
Top 10 Self-Care Tips for Helpers
1.Take Stock-What you are doing
Make a list of all the demands on your time & energy (Work, Family, Home, Health, Volunteering, other). Try to make this list as detailed as you can. Eg: Under the Work category, list the main stressors you see (number of clients, or, amount of paperwork, or difficult boss, etc). Once you have the list, take a look at it. What stands out? What factors are contributing to making your stressed out? What life situations or things you have taken on or happened to you? What would you like to change most?
2. Start a Self-Care Idea Collection
Brainstorm a list of self-care behaviors with friends and co-workers. Once you have your list, pick three ideas that jump out at you. Make a commitment to implement these in your life within the next month. Ask a friend/colleague if they would commit to supporting you (and you them) in maintaining your self care goals. This could mean that they go to the gym with you every Thursday, or that they email you at lunch to remind you to get out of your office. This is a way to stay on track and to validate your own experiences by sharing them.
3. Find time for yourself every day – Rebalance your workload
Do you work straight through lunch? Do you spend weekends running errands and catching up on your week without ever having 20 minutes to sit on the couch and do nothing? Can you think of simple ways to take mini breaks during a work day? What would work for you?
Not everyone has control over their caseload, but many do, providing they see all the clients that need to be seen. Would there be a way for you to adjust your load so that you don’t see the most challenging clients all in a row?
Make sure you do one nourishing activity each day. This could be having a 30 minute bath with no one bothering you, going out to a movie, or it could simply mean taking 10 minutes during a quiet time to sit and relax. Even small changes can make a difference in a busy helper’s life.
4. Delegate - learn to ask for help at home and at work
Are there things that you are willing to let go of and let others do their own way? Don’t expect others to read your mind: consider holding a regular family meeting to review the workload and discuss new options. Think of this: If you became ill and were in hospital for the next two weeks, who would look after things on the home front?
The same goes for work. Talk with your supervisor and co-workers about the workload that you all carry and see if you as a team can come up new paradigm shifting models to take excessive pressure off of yourself and your fellow colleagues.
5. Have a transition from work to home
Do you have a transition time between work and home? Do you have a 20 minute walk home through a beautiful park or are you stuck in traffic for two hours? Do you walk in the door to kids fighting and hanging from the curtains or do you walk into a peaceful house? Do you have a transition process when you get home? Do you change clothes? Helpers have found that their best strategies involved a transition ritual of some kind: putting on cozy clothes when getting home and mindfully putting their work clothes “away” as in putting the day away as well, having a 10 minute quiet period to shift gears, going for a run.
Do you have a transition ritual?
6. Learn to say no (or yes) more often
Helpers are often attracted to the field because they are naturally giving to others, they may also have been raised in a family where they were expected to be the strong supportive one, the parental child etc.
As helpers, we know that learning to say no is fraught with self-esteem and other personal issues and triggers. Do you think you are good at setting limits? If not, this is something that needs exploring, perhaps with a counselor. Can you think of one thing you could do to say no a bit more often?
Conversely, maybe you have stopped saying yes to all requests, because you are feeling so depleted and burned down, feel resentful and taken for granted. Have you stopped saying yes to friends, to new opportunities? Take a moment to reflect on this question and see where you fit best:
Do you need to learn to say no or yes more often?
7. Assess your Trauma Inputs
Do you work with clients who have experienced trauma? Do you read about, see photos of, and are generally exposed to difficult stories and images at your work? Take a trauma input survey of a typical day in your life.
Starting at home, what does your day begin with? Watching morning news on tv? Listening to the radio or reading the paper? Note how many disturbing images, difficult stories, actual images of dead or maimed people you come across.
Now look at your work. Not counting direct client work, how many difficult stories do you hear, whether it be in a case conference, around the water cooler debriefing a colleague or reading files?
Now look at your return trip home. Do you listen to the news on the radio? Do you watch tv at night? What do you watch? If you have a spouse who is also in the helping field, do you talk shop and debrief each other? It is important to recognize the amount of trauma information that we unconsciously absorb during the course of a day. Many helpers say that they are unable to watch much of anything on television anymore, other than perhaps the cooking channel. Others say the reverse, that they are so desensitized that they will watch very violent movies and shows and feel numb when others around them are clearly disturbed by it.
In a nutshell, there is a lot of extra trauma input outside of client work that we do not necessarily need to absorb or to hear about. We can create a “trauma filter” to protect ourselves from this extraneous material.
8. Learn more about Compassion Fatigue and Vicarious Trauma
Compassion Fatigue and Vicarious Trauma are serious, profound changes that happen when helpers do their best work. Learn more about Compassion Fatigue and Vicarious Trauma, including ways to recognize the signs and symptoms and strategies to address the problem.
Consider attending additonal workshops or read more on the topic.
9. Consider Joining a Supervision/Peer Support Group
Not all places of work offer the opportunity for peer support. You can organize such a group on your own (whether it be face to face meetings or via email or phone). This can be as small as a group of three colleagues who meet once a month or once a week to debrief and offer support to one another.
10. Attend Workshops/Professional Training Regularly
Helpers with severe compassion fatigue often speak of feeling de-skilled and incompetent. Researchers in the field of Compassion Fatigue and Vicarious Trauma have identified that attending regular professional training is one of the best ways for helpers to stay renewed and healthy. There are of course several benefits to this: connecting with peers, taking time off work, and building on your clinical skills. Identify an area of expertise that you want to grow in.
If you are not able to travel to workshops, consider taking online courses
Reference: Mathieu, Francois (2007). www.compassionfatigue.ca
|
Life Style Changes to Avoid Compassion Fatigue
Develop a Healthy Exercise Program
- Identify Benefits
- Combat Myths about exercising
- Combat Roadblocks to exercising
- Identify and overcome: Triggers to avoid, ignore, or stop exercising
- Look at what is new in exercise offerings
Benefits of Healthy Exercise
- Compensates for fat accumulation by burning calories
- Provides a "natural high'' by the release of endorphins
- Strengthens the cardiovascular and respiratory systems if aerobic type exercise sustained for at least fifteen minutes on a regular basis.
- Keeps the muscular system supple
- Keeps the circulatory system operating at its best
- Builds bone mass to combat osteoporosis.
Myths about Exercise
1. Exercise makes you tired. Because heart rate and respiration is increased, a person becomes energized, alert, and awake after a period of strenuous exercise.
2. Exercise increases your appetite. The immediate effect of exercise is a decrease in appetite
3. Exercise is boring. Rigorous exercise results in the production of hormones called endorphins which give a feeling of well-being, a "natural high
4. With exercise you can reduce certain spots on your body. Where people lose weight is determined by their hormones. With proper exercise people can increase muscle tone in certain areas and can speed along the general loss of fat, which helps overall appearance but not necessarily in specific areas.
5. You have to have athletic ability to get the most out of an exercise program. A complicated program of sophisticated athletic activities is unnecessary. Simply walking a1/2 hour to hour a day during time when you normally would have been sedentary is enough exercise to provide some balance in your life.
6. A health spa or gym is the best place to exercise. Health spas and gyms can be useful if you need a social atmosphere in which to exercise. However, the type of exercise needed for lifestyle change can be done effectively with no expense.
7. Exercise takes a lot of time and expensive equipment. You need only 30- 45 minutes of consecutive, brisk, full-body movement a day to gain the full benefit of exercise. You can do this in your home with your own equipment (e.g., stationary cycle, rebound trampoline, or rowing machine), or you can do it without equipment by walking, jump roping, etc...
Roadblocks to Exercise
- Not enough time; my schedule is already so full
- Implementing a program of exercise takes exceptional effort and planning
- The health club is too far away. It is not "on my way'' to anywhere
- An exercise program costs a lot of money.
- It is unpleasant to get all sweaty when you exercise
- Exercise can be so boring
- Exercise makes your body sore
Time for Exercise
- Make the exercise session a priority of the day
- Schedule a regular, specific time of day for exercise.
- Choose a convenient time.
- Exercise in the morning before breakfast, in the afternoon before lunch, or in the evening after getting home from work, but before dinner.
Place for Exercise
Choose an exercise easily performed around the house, e.g., treadmill, stationary cycle, rowing machine, jumping rope, rebound trampoline, jumping jacks, walking, running, biking, swimming.
Perform exercises that can be done in an air-conditioned environment (stationary cycle, rowing machine, or rebound trampoline). Profuse sweating is not necessary for exercise to be worthwhile.
Reduce Costs of Exercise
Choose an exercise which doesn't involve the purchase of equipment or club memberships, e.g., walking, running, jumping rope, etc.
Keep Exercise Interesting
Try indoor exercise in front of a TV or while listening to motivational tapes or energizing music.
lry outdoor exercise in tree-lined or park-like settings with interesting scenery and use a portable radio or tape player
For either type of exercise, get a partner or group of people to exercise with; make it a social experience that will provide mutual motivation and encouragement
Start out Slow to Protect Your Body from Being Strained
Slowly phase an exercise program in; help your body adjust to the increased activity
Use warm-up and cool-down exercises to avoid muscle strain
Wear the proper clothing and shoes to avoid body strain or injury
|
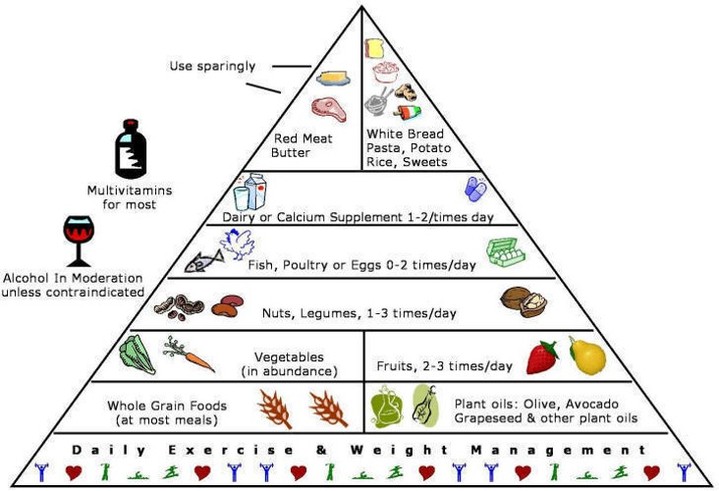
How about eating a Healthy Diet along with Exercise?
- Eat a variety of foods to get the nutrients you need & at the same time the right amount of calories to maintain healthy weight.
- Be sure to eat a balance from these food groups:
- Vegetables – as much as you want
- Fruits – 2-3 times a day
- Whole Grain Foods – at as many meals as possible
- Plant oils – such as olive, canola, corn, sunflower, peanut & other veg oils
- Nuts & Beans – 2-3 times a day
- Fish, Poultry or Eggs – 0-2 times a day
- How about eating a Healthy Diet along with Exercise?
- You need them for the vitamins, minerals, carbohydrates & protein they provide
- Pick the lowest fat choices from the food groups
- Here is a food pyramid from Harvard medical professor Walter Willett, M.D. in his book: “Eat, Drink, and be Healthy”
|
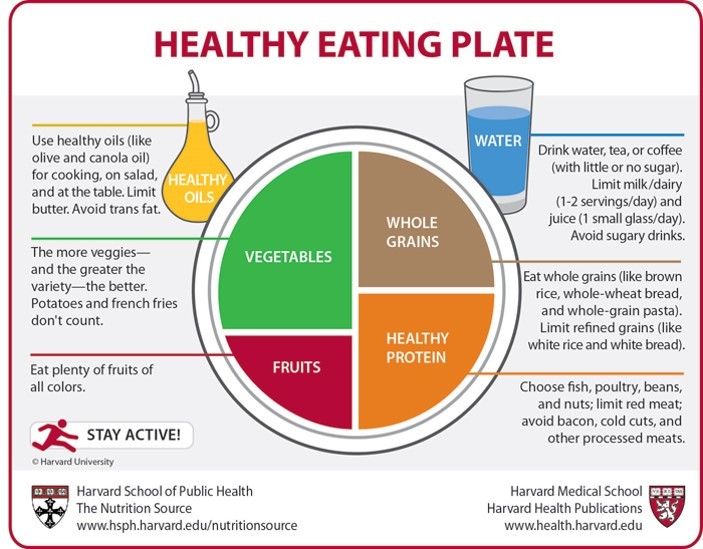
Another Version of Health Eating
To help you get the message how about using the Healthy Eating Plate Version
- Here your plate consists of:
- Lots of Vegetables
- Plenty of Fruits
- Whole Grains
- Fish, Poultry, Beans & Nuts
- A Multivitamin in your daily routine
|
Quick Guide for Healthy Eating!
Stay away from:
- Junk Foods & Sugary Drinks
- Cold Cuts & Other Processed Meats
- Bacon & Red Meats
Do make sure you
- Drink lots of sugar free Water, Tea or Coffee
- Cook with healthy oil
|
A Most Recent Word on Self-Care
In the July/August,2019 edition of The National Psychologis, Leisl Bryant, Ph.D. provided us with this most recent word on Self-Care and these strategies are essential for mental health professionals to maintain their emotional and physical health.
|
Self-care strategies for therapists:
Value and grow the person of the psychotherapist
- You will benefit from personal therapy
- Use self-awareness and self-monitoring to regularly access your own needs as carefully as you do those of your patients
- Practice Mindfulness and Self-Compassion
- Spend time learning what deeply nourishes you…and do it
- Schedule time for activities that replenish you…actually put them on your calendar and block out the time
- Set and sustain personal boundaries (both inside and outside the office)
- Acknowledge limitations and actively, thoughtfully, manage them
- Cultivate practices that nourish spiritual meaning and a sense of belonging
Refocus on reward
- Actively identify and remind yourself of the rewards of psychotherapy
- Allow yourself to experience these rewards as a means of replenishment
- Build a gratitude practice into your day
- Recognize and be realistic about professional hazards
- Understand the risks and devise strategies for managing them
- Don’t worry along, consult others
Tend the Body
- Frequently ask how you feel in your body (e.g., rest, nutrition, hydration, exercise, the need for human contact)
- Don’t wait until you’re fully depleted. Catch yourself early so you’re not working from a place of depletion
Nurture relationships both in and out of the office
- Participate in peer support/supervision groups
- Attend continuing education and colleague networking events frequently
- Meet regularly with mentors and consultants
- Make time to nurture relationships with family, friends, partners
- Have an active social life outside of work
Create a thriving environment
- Make your office a welcoming place for yourself and your patients
- Limit te number of high-risk and high-demand patients
- Get business support (e.g., administrative or virtual assistants, billing, programs/personnel)
- Actively avoid isolation if you are in private practice
- Take breaks a work
- Limit exposure to traumatic material
- Schedule vacations and time for restorative solitude and leisurely diversions
Foster your own creativity and growth
- Diversify the types of clients you see and professional services you engage in
- Actively participate in professional organizations hat are meaningful to you
- Never stop learning
|
|
So are you going to do something about it?
Make a commitment to:
1.Continuously assess your current emotional state
2.Implement a good stress reduction activity for yourself & your co-workers
3.Get 8 hours of sleep a night
4.Have a regular exercise program going for yourself & if possible your co-workers
5.Eat a good balanced diet
So there you have it!
Dealing with Compassion Fatigue is a TEAM effort which requires administration, co-workers, your families & significant others to understand that it takes a lot of effort to prevent & deal with this insidious & disabling condition!
Best of Luck!
|
References:
Abendroth, M. & Flannery, J. (2006). Predicting the risk of compassion fatigue: A study of hospice nurses. Journal of Hospice and Palliative Nursing: 8(6): 346-356.
Bride, B. (2007). Prevalence of secondary traumatic stress among social workers. Social Work: 51(2): 63-70.
Bride, B., Radey, M. & Figley, C.R. (2007). Measuring compassion fatigue. Clinical Social Work Journal: 35:155-163.
Bryant, L.M. (2019). Self-care is essential to risk management. The National Psychologist: 28(4):16.
Figley, C. R. (Ed.) (1995). Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. New York: Brunner/Mazel.
Linley, P.A. & Joseph, S. (2007). Therapy work and therapists’ positive and negative well-being. Journal of Social and Clinical Psychology: 26(3):385–403.
Mendenhall, T. (2006). Trauma-response teams: Inherent challenges and practical strategies in interdisciplinary fieldwork. Families Systems, & Health: 24(3):357-362.
Politsky, S. (2007) Revitalizing yourself. Oncology Nursing Forum: 34(2): 494.
Radey, M. & Figley, C.R. (2007). The social psychology of compassion. Clinical Social Work: 35(1):207–214
Sprang, G., Clark, J. & Whitt-Woosley, A. (2007). Compassion fatigue, compassion satisfaction, and burnout: Factors impacting a professional’s quality of life. Journal of Law and Trauma, 12:259–280.
Szabo, B. (2006). Compassion fatigue and nursing work: Can we accurately capture the consequences of caring work? International Journal of Nursing Practice: 12: 136–142.
Tehrani, N. (2007). The cost of caring – the impact of secondary trauma on assumptions, values and beliefs. Counselling Psychology Quarterly: 20(4): 325–339
Tyson, J. (2007). Compassion fatigue in the treatment of combat-related trauma during wartime. Clinical Social Work Journal; 35:183–192
Wilson, E. (2008). New program offers care for caregivers. Department of Defense Military Health System News, 23 May 2008.
|
|
|