A Short Course on Suboxone for Medication Assisted Treatment (MAT) of Opioid Use Disorder (OUD)
|
|
Dealing with the Opioid Epidemic -
A Training Resource
By Jim Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
Medication Assisted Treatment for Opioid Use Disorder
Offered by COPING.US Training Programs (CE Provider # 50-21474)
With Troy University’s Tampa Bay Site
Zoom Interactive Online Training Program
(CE Broker Tracking #: 20-790692) 3 CEU’s
This Program is approved by Florida Board of Clinical Social Work, Marriage and Family Therapy and Mental Health Counseling for: LMHC's, LMFT's, LCSW's & CMSW's
and Florida Board of Nursing for: RN's, ARNP's & LPN's
James Messina is inviting you to a scheduled Zoom meeting.
Topic: MAT Workshop
Time: Nov 18, 2020 05:30 PM Eastern Time (US and Canada)
Join Zoom Meeting
https://us02web.zoom.us/j/89967478954?pwd=b2VvbTN3bGVqZlE5K25pY1ZJc0kxUT09
Meeting ID: 899 6747 8954
Passcode: 988703
Medication Assisted Treatment for Opioid Disorder Workshop:
Wednesday November 18, 2020 at 5:30-8:30 pm via Zoom
Evaluation of Nov 18th MAT for OUD Training Workshop: Click Here
|
NEWS on Changes to the Required Waiver for Suboxone prescription use to treat OUD
The Department of Health & Human Services announced on January 14, 2021 that they have dropped the requirement for the Waiver program for buprenorphine prescriptions to remove administrative procedures widely seen as a barrier to opioid use disorder (OUD).
This change was announced on Medscape as well as on MDEdge as follows:
|
Resources for Course on coping.us
|
FOREWORD
Given that COPING.US Training Programs is providing ongoing training in MBSR Train the Trainer Certificate Programming and that we have had a desire to get these trained MBSR providers linked up with Waivered Physicians who actively prescribe suboxone in the community to their patients, I attended a 26 CEU program from the Provider Clinical Support System (PCSS) which is utilized to train medical professionals to gain a waiver to administer Suboxone to patients. In this program it was clear that to run an effective program for patients there is a need to have Behavioral Health Consultants on staff or ready for referral to assist the patients to better handle their Opioid Use Disorder and any of their other psychological issues which could impair their recovery. For this reason this Short Course is being presented on this platform to future Behavioral Health Consultants who want to enter this work.
Jim Messina, Ph.D., Director of COPING.US Training Programs. February 24, 2020
|
Background on the Opioid Crisis In American
Opioid Misuse in Primary Care
Chronic non-cancer pain highly prevalent, with substantial burdens
- Chronic pain: > 3 months
- Reported by up to 1/3 of adults
Opioids commonly prescribed for chronic pain
- 5% of U.S adults on long-term opioids
- U.S ~ 5% of world’s population, use 80% of world’s opioids (99% of hydrocodone)
Trends indicate prescribing at higher doses, more schedule II
Opioids: Potential harms to patients as well as to society
Likely under-recognized/under-diagnosed
Published rates of prescription opioid misuse among patients prescribed opioids range from 4% to 26%
One study (n=801) based on 2-hour standardized interviews
- 26% purposeful over sedation
- 39% increased dose without prescription
- 8% obtained extra opioids from other doctors
- 18% used for purposes other than pain
- 20% drinking alcohol to relieve pain
- 12% hoarded pain medications
Definitions inconsistent across studies and behaviors evaluated vary in seriousness
Poorly standardized methods to detect these outcomes
Data from efficacy trials underestimate risks
(Fleming, M.F. et al. (2007). Substance use disorders in a primary care sample receiving daily opioid therapy. Journal of Pain, 8,573-82)
|
Factors Associated with Opioid Overdose in Patients Prescribed Opioids
Aberrant behaviors
- Extra doses, unauthorized dose escalation, lost prescriptions, after-hours refill requests, obtaining opioids from multiple prescribers, using unprescribed opioids or other medications/substances, use to treat non-pain symptoms
Recent initiation of opioids
Receipt of methadone as an analgesic
Concomitant use of benzodiazepines
Substance use disorder
Psychological comorbidities
Higher opioid doses
Universal Precautions in Pain Medicine
Why utilize universal precautions?
Predicting opioid misuse is imprecise
- Protects all patients
- Protects the public and community health
Consistent application of precautions
Consistent with clinical practice guidelines
- Takes pressure off provider
- Reduces stigmatization of individual patients and bias in management
- Standardizes systems of care
Universal precautions provide a standardized approach while allowing for individualized assessment and management decisions
Common Universal Precautions
Comprehensive pain assessment including opioid risk assessment
Formulation of pain diagnosis/es
Initial opioid prescription should be considered a test or trial; continue or discontinue based on ongoing reassessment of risks and benefits
- Decision to continue or discontinue opioid therapy should be made regularly (e.g., every 2-3 months)
Regular face-to-face visits
Clear documentation
Mitigating Risks Associated with Opioids
Careful patient assessment and selection
Medication agreements
Avoid higher doses
Monitoring, including urine drug testing
Review prescription drug monitoring data (States’ Prescription Drug Monitoring Plan - PDMP)
Avoid sedative-hypnotics (particularly benzodiazepines)
Addiction, pain, or psychiatric consultation
More frequent refills with smaller quantities
Abuse-deterrent formulations
Naloxone co-prescription
Evidence on effects of risk mitigation strategies on clinical outcomes (overdose, OUD) is lacking
|
Patient Selection and Risk Stratification
Risk assessment in all patients prior to initiating opioids
Aberrant drug-related behaviors in up to 50% of patients prescribed opioids for chronic pain
- Strongest predictor personal or family history of alcohol or drug abuse
- Psychological comorbidities also a factor
Only consider opioids in patients in whom benefits likely outweigh risks
- Opioids are not always appropriate
Tools for risk stratification available
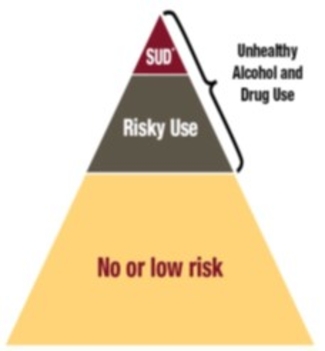
Screening for Unhealthy Substance Use Disorders (SUDS)
|
Alcohol
“Do you sometimes drink beer, wine or other alcoholic beverages?”
“How many times in the past year have you had 5 (4 for women) or more drinks in a day?”
(positive: > never)
Drugs
“How many times in the past year have you used an illegal drug or used a prescription medication for non-medical reasons?”
(positive: > never)
Opioid Misuse Risk Screening Tools
ORT: Opioid Risk Tool
SOAPP: Screening & Opioid Assessment for Patients with Pain
COMM: Chronic Opioid Misuse Measure
STAR: Screening Tool for Addiction Risk
SISAP: Screening Instrument for Substance Abuse Potential
PDUQ: Prescription Drug Use Questionnaire
No “gold standard” and Lack rigorous testing
|
Medication Agreements
Informed consent (goals and risks)
Plan of care
- Goals of therapy
- Follow-up and monitoring plan
- How opioids will be prescribed and refilled
Signed by both patient and prescriber
Serves as a patient counseling document and delineates expectations
Documents plan of care for other clinicians
Evidence on effects on clinical outcomes lacking
Initiation and Titration of Opioids
View initial course of opioids as a short-term (e.g., 4 weeks), therapeutic trial
- The decision to proceed (or continue) with Long-acting Opioid treatment (LOT) should be a conscious one
- If opioids are used, should be part of a multimodal strategy
Start at low doses and titrate cautiously
Do not initiate therapy with long-acting opioid
- Insufficient evidence to recommend that all patients be transitioned to round-the-clock, long-acting opioids
Methadone and fentanyl not recommended as first line options
- Less predictable and more complicated dosing and pharmacokinetics
- Buprenorphine is a partial agonist with theoretically lower respiratory risk and might be useful in higher-risk patients; evidence showing decreased overdose risk is lacking and some formulations not approved for chronic pain (only approved for OUD)
Dosing
No theoretical ceiling with opioids
- Benefits of higher doses unclear, since questions arise due to opioid non-responders
- Titration to achieve pain relief inconsistent with evidence on benefits
- Dose-related risk of overdose
Dose thresholds
- 2016 CDC guideline: “Caution” at doses >50 MED/day and “avoid” doses >90 MED/day
- Average dose in overdoses 98 MED/day
- 50% of overdoses in patients on <60 MED/day
- If higher doses used, need for more frequent or intense monitoring and additional risk mitigation strategies
Monitoring Outcomes
Evaluate patients in multiple domains
- Focus away from pain as the main goal of treatment
- No therapy for chronic pain is effective in completely relieving pain
- Patients can report improvement in pain with no improvement in function
- Measure function and set functional goals
- Achievable, measurable
- Screen for psychological comorbidities
- Assess sleep issues
- Screen for substance abuse
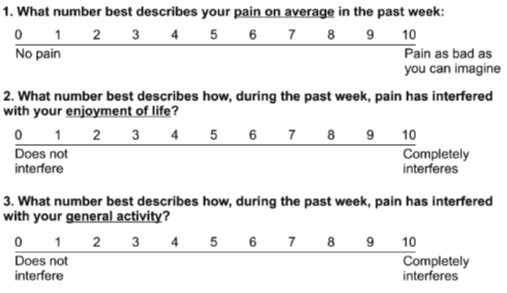
Screen for Level of Pain using the PEG Scale
|
Urine Drug Tests
Provides objective information regarding:
- Self-report unreliable and behavioral observations detect only some problems
- Evidence of adherence to opioid plan of care
- Evidence of use or non-use of illicit substances or unprescribed medications
- May improve adherence
Perform at baseline and periodically
- 1-2 times/year for low-risk patients; 3-4 times/year for higher risk
- Random, scheduled, and /or when concerns arise
- Discuss expected findings with patient prior to testing
- Consult with toxicologist/clinical pathologist before acting if patient disputes findings
- Screening tests requires confirmation
- Dedicated deceivers can beat the system
Prescription Drug Monitoring Programs
Available now in almost all states
Use of PDMPs can identify cases of doctor shopping
Use of PDMPs variable and generally suboptimal
PDMPs vary in who can access, information not available across states
>20 states mandate use before writing for controlled substances (as of June 2014)
Evidence showing effects of PDMP monitoring on clinical outcomes (overdose, OUD) lacking
|
Avoid Opioids and Benzo’s
Concomitant benzodiazepine use associated with markedly increased risk of opioid overdose
- Other medications with respiratory depressant effects may also be associated with similar risks
Taper benzodiazepines gradually
Offer evidence-based psychotherapies for anxiety
- Cognitive behavioral therapy
- Anti-depressants approved for anxiety
- Other non-benzodiazepine medications approved for anxiety
Coordinate care with mental health professionals
Naloxone – “Narcan”
Opioid antagonist that can rapidly reverse opioid overdose; most overdose episodes are witnessed
- Highly effective in addiction settings
- Some evidence of effectiveness in chronic pain settings
CDC recommends for all patients on ≥50 MED/day, or other risk factors for overdose
- Consider for all patients prescribed opioids
All states have passed Good Samaritan laws providing civil or criminal immunity for administration of naloxone
- Resources/education: http://prescribetoprevent.org/
Available in FDA-approved IM and IN formulations, also used off-label
Abuse-Deterrent Formulations
Abuse-deterrent formulations recently approved by FDA or undergoing FDA approval process
- Designed to be tamper-resistant or co-formulated with medications that reverse opioid effects or produce noxious side effects when tampered with
- Effectiveness for reducing misuse/substance abuse and improving clinical outcomes unproven
- Likely to be primarily effective in patients who crush or inject opioids
- Some patients may seek other prescription or illicit opioids
Evaluation of Aberrant Drug-Related Behaviors
Always evaluate aberrant drug-related behaviors
- Behaviors vary in seriousness
- Need to judge seriousness, the cause or causes, likelihood of recurrence, and clinical context
- Predictors of high likelihood of future aberrant behaviors include 3 or more episodes of aberrant behaviors and sense of “losing control”
- Serious behaviors include diversion, injecting oral drugs
- Responses range from patient education and enhanced monitoring to referral to addiction specialist and discontinuation of therapy
Discontinuation of Opioid Therapy
Taper or wean patients off of long-term opioid therapy [LOT] when they:
- Engage in serious or repeated aberrant drug-related behaviors or drug abuse/diversion
- Experience no progress towards meeting therapeutic goals
- Experience intolerable adverse effects
Continue to manage pain off opioids
Have an exit strategy when initiating a trial of LOT
- Indications for stopping LOT
- Plans for tapering or discontinuing
- Reduction in daily dose of 10% per week reasonable starting point
- Some patients may require slower tapers
- Know resources for managing addiction and mental health issues
Patients Already on High Doses
For established patients on >90 MME/day who meet criteria for taper, initiate taper!
For patients who do not meet criteria for taper
- Discuss recent evidence regarding dose-dependent overdose risk
- Re-evaluate continued use of high opioid dosages
- Offer opportunity to taper
Collaborate with the patient on a tapering plan
|
Background on Opioid Use Disorder
Defining Substance Use Disorder
Primary, chronic brain disease characterized by compulsive substance seeking and use despite harmful consequences
Involves cycles of relapse and remission
40-60% genetic
Defining Chronic Illness
Long in duration—often with protracted clinical course
Associated with persistent and recurring health problems
Multi-factorial in etiology, often heritable
No definite cure
Requires ongoing medical care
SUD Meets Criteria for Chronic Illness
Common features with other chronic illnesses:
- Heritability
- Influenced by environment and behavior
- Responds to appropriate treatment
- Without adequate treatment can be progressive and result in substantial morbidity and mortality
- Has a biological/physiological basis, is ongoing and long term, can involve recurrences
Treatment and Outcomes Similar to Other Chronic Illnesses
Treatment outcomes as good as other chronic illnesses
Relapse or recurrence rates similar
Adherence and engagement crucial
What are Effective Treatment for SUDS?
Pharmacotherapy
Alcohol use disorder
- naltrexone, acamprosate, disulfiram, topiramate*
Opioid use disorder
- methadone, buprenorphine, naltrexone
Tobacco use disorder
- varenicline, bupropion, NRT
Cocaine use disorder
Psychosocial/behavioral
Levels of care
- Outpatient, IOP/PHP, residential
Modalities
Recovery Supports
- Mutual help/peer support
- Recovery coaching
Similar to Medical Management of Other Chronic Illnesses (e.g. Diabetes or HIV)
No cure
Goal is prevention of acute and chronic complications
Individualized treatment plans and targets
Treatment includes:
- Medication
- Lifestyle changes
- Regular monitoring for complications
- Behavioral support
How Long Should Treatment Last?
“In most cases, treatment will be required in the long term or even throughout life. The aim of treatment services is not only to reduce or stop opioid use, but also to improve health and social functioning, and to help patients avoid some of the more serious consequences of drug use. Such long-term treatment, common for many medical conditions, should not be seen as treatment failure, but rather as a cost-effective way of prolonging life and improving quality of life, supporting the natural and long-term process of change and recovery.”
Why Does SUDS Care Look so Different?
WHO study of 18 most stigmatized social problems in 14 countries:
- Drug addiction ranked number 1
- Alcohol addiction ranked number 4
Stigma associated with poor mental and physical health among people who use drugs
Stigma among top reasons people don’t access treatment
|
What is Stigma?
Attribute, behavior, or condition that is socially discrediting
Two main factors influence stigma:
- Cause and controllability
- Stigma decreases when:
− “It’s not his fault”
− “She can’t help it”
Stop Talking Dirty: Getting Rid of “Substance Abuse”
Abuse: Derived from word meaning “wicked act or practice, a shameful thing, a violation of decency”
Associated with behavior such as rape, domestic violence, and child molestation
Professionals more likely to view patient as deserving of punishment if described as a “substance abuser”
Types of Stigma for SUDs
Stigma from within
- Blame self, feel hopeless
Stigma from recovery community
- Medications versus “abstinence”
Stigma from clinicians
- Belief that treatment is ineffective
Stigma from outside
Examples of Stigma
People with SUD and those on agonist therapy may not be accepted to post-acute care facilities
People on agonist therapy may not be offered organ transplantation
People mandated to treatment as a condition of probation who have a positive toxicology despite treatment adherence can be imprisoned
Impact of Stigma
Erodes confidence that substance use disorder is a valid and treatable health condition
Barrier to jobs, housing, relationships
Deters public from wanting to pay for treatment, allows insurers to restrict coverage
Stops people from seeking help
Impacts clinical care and treatment decisions
Change Language to Improve Care:
Avoid: “dirty,” “clean,” “abuse,” and “abuser”
Consider changing: Medication Assisted Treatment
- Medications for addiction treatment are life-saving similar to insulin for diabetes, which is not called “insulin assisted treatment” despite importance of behavioral interventions with diabetes care
“Medically supervised withdrawal" also more accurate and less stigmatizing than "Detox"
Terminology related to Opioid Use Disorder
Unhealthy use
Binge
- Heavy episode
- Multiple days
Disorder
Dependence
- Physical
- Addiction
- ICD-10-CM, DSM 5 and prior
Misuse
Return to use
- Recurrence
- Remission
- Relapse
Medication
- Substitution
- Assisted
- Replacement
|
The Need for Change
“For nearly a century, physicians were indoctrinated with the societal attitude that addicts brought upon themselves the suffering they deserve. Even after we began to regard addicts as having a disease, our policies continued to reflect our attitude: addicts are sick, they need help, but they also sin, so do not help them too much. Until the correct mindset is restored in the physician, the mere availability of an effective medication will not make a difference. To put it another way, for buprenorphine to succeed clinically, physicians themselves must first change before they can help patients change their lives.”
Opioid Use Disorder (OUD)
DSM-5: “A problematic pattern of opioid use leading to clinically significant impairment or distress”
2014: 1.9 million Americans with OUD due to prescription drugs, ~600,000 due to heroin
OUD: Decreased quality of life, negative impacts on morbidity and mortality
Treatment:
- FDA-approved medications: agonist (methadone), partial agonist (buprenorphine), antagonist (naltrexone)
- Block euphoric, sedating effect, decrease craving, mitigate withdrawal
- Decrease illicit use and misuse of medication, improves social functioning
- Decrease criminal activity, risks associated with injection drug use
DSM-5 Criteria for OUD
Mild OUD: 2-3 Criteria
Moderate OUD: 4-5 Criteria
Severe OUD: >6 Criteria
- Tolerance
- Withdrawal
- Use in larger amounts or duration than intended
- Persistent desire to cut down
- Giving up interests to use opioids
- Great deal of time spent obtaining, using or recovering from opioids
- Craving or strong desire to use opioids
- Recurrent use resulting in failure to fulfill major role obligations
- Recurrent use in hazardous situations
10. Continued use despite social or interpersonal problems caused or exacerbated by opioids
11. Continued use despite physical or psychological problems
Suspected Opioid Use Disorder
Discuss with your patient and provide an opportunity to disclose concerns.
Assess for OUD using DSM-5 criteria. If present, offer or arrange medication assisted treatment [MAT].
- Buprenorphine through an office-based buprenorphine treatment provider or an opioid treatment program specialist
- Methadone maintenance therapy from an opioid treatment program specialist
- Oral or long-acting injectable formulations of naltrexone (for highly motivated non-pregnant adults)
Physicians with patients with suspected OUD, should consider obtaining a waiver to prescribe buprenorphine for OUD (see http://www.samhsa.gov/medication-assisted-treatment/buprenorphine-waiver-management ) and PCSS waiver offerings
|
Major Source of Opioid Use Disorder:
Aftermath of Treating PAIN
Opioids for Acute Pain
Opioids generally considered effective for acute pain
- But, recent data indicates that opioids may be no more effective than a Nonsteroidal Anti-inflammatory Drug (NSAID) alone for acute pain
Use of opioids for “minor” pain associated with increased risk of long-term use
- Versus no opioid use, opioid within 7 days of minor surgery associated with 44% increased risk of use at 1 year
Prescribing excessive quantities of opioids for acute pain resulting in leftover opioids
- Source of diversion and unprescribed use
More judicious use of opioids for acute pain
- If used, limit opioids to a 3-7 day supply for most acute pain
Opioids for Chronic Pain
Opioids moderately more effective than placebo for short-term pain relief
- Effects average 20-30% improvement in pain, 1-2 points vs. placebo
Data on long-term effectiveness limited
- Until recently, no placebo-controlled trials >6 months, most trials <8 weeks
- Uncontrolled studies indicate many discontinuations due to adverse effects (23%) or insufficient pain relief (10%), some patients who continued on opioids experienced long-term pain relief
Effects on function generally smaller than effects on pain, some trials showed no or minimal benefits
Optimal results—trials excluded patients at high risk for abuse/misuse, psychological or serious medical comorbidities
Limited evidence on commonly treated conditions
- Fibromyalgia, headache, others
|
|
Opioids: Suffering from Our Treatment of Pain*
• Opioid prescribing has almost doubled since the late 1990’s due to pain treatment initiatives and guidelines. Opioid use disorders are highly related to increased health care utilization costs.
• Opioids were involved in 33,091 deaths in 2015, and opioid overdoses have quadrupled since 1999.
• 60% of drug overdose deaths are related to pharmaceuticals and 75% include prescription opioids.
• Tightening of opioid prescribing trends has been correlated with increased heroin use and heroin overdose.
• Long-term preventive care decreases costs on high opioid-related emergency room utilization rates.
• 23.5 million people are estimated to need substance use disorders treatment, yet only 2.6 million receive it. Nationwide, there are under 40,000 prescribers for buprenorphine, which is estimated to be far below the national access needs; less than half of the 2.2 million people who need treatment for opioid use disorders receive it.1
• Results from a 2005 congressionally mandated evaluation study show that in-office MAT has increased the availability of treatment for opioid dependence; treatment is generally safe and effective; diversion, adverse clinical events, and public health consequences have been minimal.
* National Association of Community Health Centers. (2018). Business plan for medication assisted training. Providers Clinical Support System (PCSS) at: https://pcssnow.org/resource/business-plan-for-medication-assisted-treatment-mat/
|
|
2016 CDC Guidelines Concerning use of Opioids for Pain
Recommendation #1 (chronic pain)
- Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain.
- Consider opioid therapy only if expected benefits are anticipated to outweigh risks to the patient.
- If opioids are used, combine with appropriate nonpharmacologic therapy and nonopioid pharmacologic therapy.
Recommendation #6 (acute pain)
- When opioids are used for acute pain, prescribe the lowest effective dose of immediate-release opioids and prescribe no greater quantity than needed for expected duration and severity of pain (usually 3 to 7 days)
Approach to Treatment of Pain
Acute pain
- Avoid prescribed bed rest, early return to activity as able, heat/cold, OTC analgesics
- Identify and address psycho-social risk factors early to help prevent transition to chronic pain
Chronic pain
- Focus on functional goals and improvement, not just pain
- Self-care (coping skills, relaxation/meditation, activity/exercise)
- Identify and address psychosocial contributors to pain
−Depression, anxiety, PTSD
−Sleep issues
Non-Opioid Therapies for Pain
A number of non-opioid therapies are similarly or more effective than opioids, and safer
- Opioids ≠ effective/good pain management
Prioritize active over passive modalities
- Biopsychosocial understanding of chronic pain
- Active therapies: Psychological treatments, exercise, interdisciplinary rehabilitation, mind-body interventions
−Actively engage patients with focus on improving function
Passive therapies: Medications, physical modalities, complementary and alternative treatments, interventional treatments
- Main focus is symptom relief
- Use as an adjunct or bridge to active therapies
Costs, availability, patient adherence
Cognitive Behavioral Therapy
Psychological therapy that integrates:
Cognitive therapy
- Restructures maladaptive thinking patterns
Behavioral therapy
- Replace undesirable with healthier behaviors
Effective for improving pain, disability, mood, maladaptive behaviors
- Some effects appear sustained
- More effective in persons with psychosocial risk factors
Meditation/Relaxation
Helpful technique for self-management and coping
- Incorporates some CBT principles
Distraction, reduce anxiety, reduce sympathetic arousal, reduce muscle tension, altered central processing
Evidence on effectiveness increasing
- Mindfulness-based Stress Reduction similarly effective to CBT
Varied techniques
- Meditation
- Progressive muscle relaxation
- Hypnosis
- Guided imagery
- Yoga, Tai Chi—movement-based therapies that incorporate meditation or relaxation principles
- Related: Biofeedback
Exercise
Effects on pain and function (and general health!)
- Impact on fear avoidance behaviors (hurt does not equal harm)
Many different types for exercise
- Aerobic, strengthening, stretching, mixed
- McKenzie, motor control and stabilization, active trunk exercise, others
- Supervised vs. home, group vs. individual
- Related: Alexander technique, Pilates, yoga, Tai Chi, others
Ideally done within a CBT-informed framework
No technique clearly superior
- Supervised, individualized exercise programs more effective initially?
- Handouts and videos for home exercise
- Start slow, incremental increases; goal is sustained engagement
Interdisciplinary Rehabilitation
Combines at a minimum psychological treatments and exercise
- Provided by professionals from at least two different specialties
- Focus on improvement in function
Components and intensity of interdisciplinary rehabilitation vary
More effective than non-interdisciplinary rehab, some evidence of sustained effects
Lack of availability and reimbursement important barriers
- May be most effective in persons who fail standard therapies, severe functional deficits, severe psychosocial risk factors
Passive Therapies
Physical modalities: Evidence limited and difficult to show consistent or sustained benefits
- Heat similarly effective to NSAIDs for acute LBP
- Other modalities not generally recommended
Manipulation, acupuncture, massage: Some evidence of benefit for certain pain conditions
- Some effects likely non-specific and related to “hand-on” nature
- If used, as adjunct to active therapies
- Be aware of costs and discontinue if ineffective in initial trial
- Expectations of benefit can predict effectiveness
- Enhanced access to complementary and alternative therapies through the Affordable Care Act
Medications
Acetaminophen and NSAIDs first-line therapies for many conditions; benefits modest
Tramadol and tapentadol: Dual mode of action (opioid receptor and centrally acting); tramadol schedule IV and tapentadol schedule II
Gabapentin and pregabalin: First line for neuropathic pain (pregabalin schedule V); off-label for non-neuropathic pain
Antidepressants: SNRI’s first line for neuropathic pain; TCA’s with anticholinergic and cardiac AE’s
- Duloxetine approved for fibromyalgia and chronic back pain
Skeletal muscle relaxants: Sedating, short-term use for acute pain
- Cyclobenzaprine (similar to TCA) and tizanidine (similar to clonidine) best-studied
Benzodiazepines: Avoid!
Topical lidocaine for neuropathic pain, topical NSAIDs for localized OA
Conclusions
- Very limited data on long-term benefits of opioid therapy, with some evidence showing no benefits versus non-opioid therapy
- Accumulating evidence on serious harms of long-term opioid therapy that appear to be dose-dependent
- Benefits appear limited and harms are significant, suggesting a close balance of benefits to harm
- A more cautious approach to use of opioids for pain is indicated
- Universal precautions, including risk assessment, patient selection, monitoring, and risk mitigation strategies
- Non-opioid therapies preferred
- Assess for and treat opioid use disorder; training for prescribing buprenorphine in office-based settings available
|
Background on Medical Providers for the Opioid Crisis
Becoming an OUD Medication Treatment Provider
SAMHSA strongly urges physicians, NPs, and PAs to obtain waivers that will qualify them to offer buprenorphine pharmacotherapy. They can become qualified to use buprenorphine to taper appropriate patients with OUD off illicit or prescription opioids or to provide long-term OUD treatment.
Only healthcare professionals with a federal waiver may prescribe buprenorphine for the treatment of OUD. To get waivers, providers must meet set criteria, complete buprenorphine training (online or in person), and apply for a waiver from SAMHSA. Waivered prescribers are assigned an additional DEA registration number (usually their existing number with an added “X”). NPs and PAs need to meet additional criteria for waivers.
Check with the state licensing board about restrictions and requirements at the state level before applying for a waiver.
Waiver training: ASAM, the American Academy of Addiction Psychiatry, the American Psychiatric Association, and the American Osteopathic Academy of Addiction Medicine all provide the waiver training courses for physicians. Providers’ Clinical Support System for Medication Assisted Treatment (PCSS-MAT) provides the required 8-hour OUD medication waiver course for physicians and 24-hour waiver course for NPs and PAs for free (https://pcssmat.org /education-training/mat-waiver-training). ASAM and others also provide NP and PA courses.
New prescribers can benefit from mentorship from experienced providers in their practice or community. Mentorship is available for free from PCSS-MAT (http://pcssmat.org/mentoring).
.
|
|
Patient Loads Allowed under the DATA 2000 Waiver Plan*
Each DATA 2000-waivered physician can see 30 active patients for the first year of registration and up to 275 patients by the start of the third year participating in buprenorphine Medication-Assisted Treatment (MAT) for opioid use disorders.
Each DATA 2000-waivered physician assistant or nurse practitioner can see up to 30 active patients.
*National Association of Community Health Centers. (2018). Business plan for medication assisted training. Providers Clinical Support System (PCSS) at: https://pcssnow.org/resource/business-plan-for-medication-assisted-treatment-mat/
|
|
How to find a Medical Practitioner who has the waiver to administer Suboxone
There are two sites on which you can find Practitioners who have the waiver to administer suboxone.
2. SUBOXONE.IO an international website which provides names of providers who have the Suboxone waiver at: https://buprenorphine.io/
|
|
Funding for Counselors within Suboxone Treatment Centers
Support for Patients and Communities Act (H.R. 6), commonly referred to as “The Support Act,” has expanded the definition of allowable mental health care services under Provision B to include LMHCs and LPCs operating within certified Opioid Treatment Programs (OTP) for the purpose of Opioid Use Disorder (OUD) treatment. The work of licensed mental health and professional counselors in opioid treatment programs certified by the Substance Abuse and Mental Health Services Administration (SAMHSA) was eligible for Medicare reimbursement as of Jan. 1, 2020. This reimbursement will be made only to the opioid treatment programs and not to individuals.
|
|
Background on MAT for OUD
Purpose of Medication for Opioid Use Disorder (OUD)
Allow reestablishment of homeostasis of the reward pathways in the brain away from substances
- Restore emotional and decision-making capacities
- Control symptoms of opioid withdrawal
- Suppress opioid cravings
- Block the reinforcing effects of ongoing opioid use
- Promote and facilitate patient engagement in recovery-oriented activities
Coupled with behavioral interventions
- Enhance the salience of natural, healthy rewards
- Reduce stress reactivity and negative emotional state
- Improve self-regulation
- Increase avoidance of relapse triggers
Goals of Medication for Opioid Use Disorder (OUD)
- Reduce mortality - All cause and drug-related
- Reduce associated morbidity e.g: Transmission of blood-borne viruses and Infectious complications from IV drug use
- Reduce and/or discontinue opioid use
- Increase retention in addiction treatment
- Improve general health and well-being
- Reduce drug-related crime
Should medications be used in the treatment of addiction?
- Is this a scientific question?
- Is this a philosophical question?
- Is this a practical question?
Rationale for medication
- Impact the physiology of addiction and dependence
- Improve outcomes including retention and opioiduse
- Protect against lapses, which should be expected
- Reduce high rates of relapse
- Without medications >80% of heroin addicts relapse within 30 days after detoxification
Medication for Opioid Use Disorder (OUD)
1. Methadone – Full Agonist (See Note below)
2. Buprenorphine – Partial Agonist - Subutex
- Office-Based
- Opioid Treatment Program
3. Naltrexone – Antagonist - Vivitrol
- Office-Based
- Opioid Treatment Program
4. Buprenorphine & Naloxone-Combination Agonist & Antagonist - Suboxone, Zubsolv, Bunavail
- Office-Based
- Opioid Treatment Program
For Overdoses Naloxone – Antagonist - Narcan
NOTE: An agonist is a chemical that binds to a receptor and activates the receptor to produce a biological response. Whereas an agonist causes an action, an antagonist blocks the action of the agonist and an inverse agonist causes an action opposite to that of the agonist.
- Counseling mandatory for methadone; ability to refer to counseling necessary for buprenorphine; optional for naltrexone but encouraged.
- All medical modalities require medication management
Difference between Suboxone and Subutex
Both Suboxone and Subutex contain the same active ingredient, a substance called buprenorphine. In medical terminology, buprenorphine is known as an “opioid partial agonist.” This means that buprenorphine interacts with the same receptors in the brain that are affected by opiates such as heroin and oxycodone — but without causing the disorienting high that results from opiate abuse. Because of this, individuals who take Suboxone or Subutex under proper professional supervision can live their lives without experiencing the cravings that would normally occur in the absence of the opiate to which they had become addicted.
Because the buprenorphine “tricks” the brain into believing that it has encountered an opiate, Suboxone and Subutex patients also avoid going through withdrawal.
The primary difference between Suboxone and Subutex is that one of these medications also contains a substance called “naloxone.” while the other one does not:
- Subutex contains a single active ingredient: buprenorphine.
- Suboxone contains two active ingredients: buprenorphine and naloxone.
Naloxone is added to the formulation to keep people from abusing the medication. For example, if a person was high on heroin and took an intravenous dose of naloxone, they would crash into an immediate state of opiate withdrawal. Naloxone works as an opiate antagonist. It will fill the opiate receptors in the brain and it won’t let other drugs activate these receptors, but unlike buprenorphine (which fills and activates receptors) naloxone will not activate opiate receptors. With all receptors full but not activated, a person feels immediate and intense withdrawal pains.
Rationale for Buprenorphine/Naloxone Combination
Naloxone present in attempt to decrease misuse or diversion
Naloxone is mostly inactive unless injected
- Very low bioavailability of naloxone when medication used sublingually
- If patient opioid dependent and not in opioid withdrawal, injection of buprenorphine/naloxone can precipitate withdrawal
- If patient in opioid withdrawal, injection of buprenorphine/naloxone can have euphorogenic or opioid withdrawal relieving effects
|
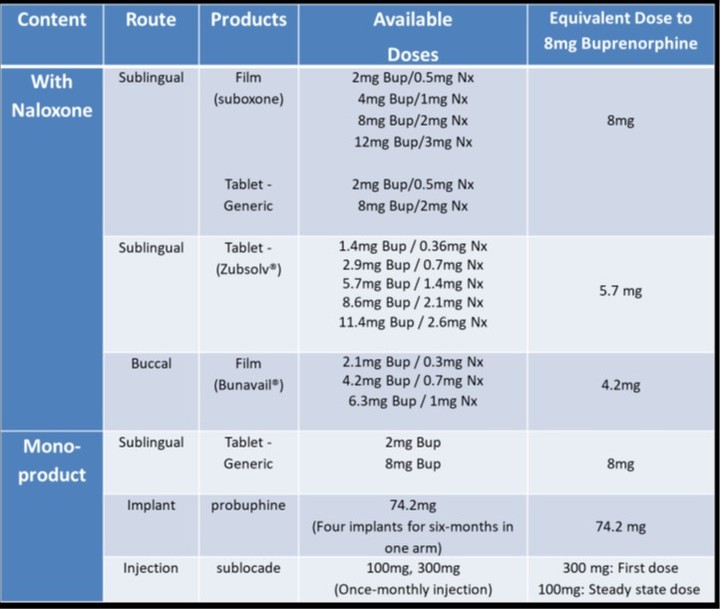
Commercially Available Transmucosal Buprenorphine Formulations
for the Treatment of OUD
|
|
Buprenorphine/
Naloxone
|
Suboxone®
|
Buprenorphine
|
Zubsolv®
|
Bunavail®
|
|
Formulation
|
SL Tablets
SL = sublingual
|
SL Film
SL = sublingual
|
SL Tablets
SL = sublingual
|
SL Tablets
SL = sublingual
|
Mucous Membrane Film
|
|
Dosages Available
|
2/0.5mg
8/2mg
|
2/0.5mg
4/1mg
8/2mg
12/3mg
|
2mg
8mg
|
1.4/0.36mg
2.9/0.71mg
5.7/1.4mg
8.6/2.1mg
11.4/2.9mg
|
2.1/0.3mg
4.2/0.7mg
6.3/1mg
|
|
Concomitant Naloxone
|
Yes
|
Yes
|
No
|
Yes
|
Yes
|
|
Buprenorphine Implant (Probuphine®)
FDA approved in 2016
Indication: Treatment of OUD in patients who have been clinically stabilized on transmucosal buprenorphine 8 mg/day or less.
Medication consists of 4 implants (80mg/implant) surgically inserted into the subdermal region of the upper arm that release buprenorphine for 6 months.
At steady state (after 4 weeks), comparable to trough buprenorphine plasma levels produced by daily sublingual buprenorphine doses of 8mg or less.
To prescribe, insert or remove medication, providers must complete a live training program.
Buprenorphine Depot Injection (Sublocade®)
FDA approval obtained November 2017
Moderate to severe OUD treatment
Monthly subcutaneous abdominal injection
- Minimum 7 days of transmucosal buprenorphine treatment first
Two doses
- 300mg/1.5mL and 100mg/0.5mL
Two dosing options based on current evidence
- 300mg/1.5mL x 6 months
- 300mg/1.5mL x 2 months, followed by 100mg/0.5mL x 4 months
Peak buprenorphine concentrations occur ~24 hrs after injection
Steady state achieved in 4 to 6 months
After discontinuation, patients may have detectable plasma levels for 12 months or longer
Oral Naltrexone
Opioid antagonist: blocks all opioid receptors
Two formulations: Oral and Intramuscular
Oral Naltrexone FDA approved in 1984 for blockade of effects of administered opioids
- Dose is 50mg daily
- Alternative dosing = dose three times a week with two 100mg-doses followed by 150mg dose
- Not widely used to treat OUD because low rates of patient acceptance, difficulty with initiation, and high rates of medication nonadherence
Cochrane Review did not find oral naltrexone superior to placebo or no medication in treatment retention and illicit opioid use
Extended-Release (XR) Naltrexone: Intramuscular Injection
FDA approved 2010 for treatment of opioid use disorder following medically supervised withdrawal
380mg administered intramuscularly once every 4 weeks
- Some people may metabolize quickly and need injection in 21 days
Consider in
- Patients who have failed agonist treatment
- Patients confined to environments that do not allow for medication treatments
- Patients who do not have access to agonist treatment
- Patients with high risk of diversion
- Patients who are highly motivated and willing to taper off opioid agonists
- Patients who do not want to be treated with an agonist
- Patients with concomitant opioid and alcohol use disorder
XR-Naltrexone
Requires patient to be fully abstinent from opioids
- Short acting opioids = 5-7 days abstinent
- Long acting opioids = 7-10 days abstinent
- Confirm opioid abstinence with urine drug test and/or naloxone challenge
Few drug-drug interactions
Induction delays and non-adherence may reduce overall effectiveness
What is Medication Management?
Treatment of opioid withdrawal
Medication initiation
Evaluation for safety and effectiveness
Confirmation of adherence
- Urine drug testing, pill counts, patient report
Evaluating treatment plan based on patient need and adherence
Referral for or treatment of mental illness, if needed
Also involves
- Psychosocial needs assessment
- Supportive counseling
- Case management
- Links to existing family supports
- Referral to community services
Role of Counseling
Purpose:
- Modify behaviors that maintain or reinforce drug use
- Develop coping strategies
- Encourage medication adherence
- Treat or identify concomitant mental illness that can complicate SUD or trigger relapse
Some evidence shows that psychosocial treatment improves adherence and retention in treatment, but findings are mixed
Effective Counseling Modalities
Relationship building
Cognitive behavioral therapies
Contingency management
Relapse prevention
Motivational interviewing
|
|
About Medication-Assisted Treatment (MAT)*
Used as a harm-reduction model and evidence-based treatment for patients who already suffer from opioid use disorder.
Goals include:
1. A decrease symptoms of opioid use disorder (such as illicit opioid use)
2. Decreased mortality
3. Reductions in criminal activity.13
It is recommended that MAT be offered in conjunction with psychosocial supports, which may include:
1. Alcohol and Other Drugs of Abuse (AODA) counseling
2. Psychotherapy
3. Referral to social services such as employment and education assistance
* National Association of Community Health Centers. (2018). Business plan for medication assisted training. Providers Clinical Support System (PCSS) at: https://pcssnow.org/resource/business-plan-for-medication-assisted-treatment-mat/
|
|
Background on Set up of Office Based MAT Program
for OUD
Office-Based Opioid Treatment
Pharmacologic:
Buprenorphine-naloxone prescribed during office visits
Coordination/Integration of Care:
Some practices designate clinic staff member as coordinator
Education/Outreach:
DATA 2000 waiver training
Access to PCSS
Psychosocial:
On-site brief counseling by physician or other staff
Off-site referrals
Integrating Buprenorphine into Clinical Practice
Preparing the Whole Team
- Front desk/phone room staff
- Medical assistant
- Nurse
- Physicians
- Counselor
- Clinic medical director
Designate a coordinator (“the glue person”)
OK to start small and slow – just start!
Who Does What?
Front desk/phone room staff
- Scheduling, face/voice of practice
Medical Assistant or Nurse
- Measure Clinical Opioids Withdrawal Scale (COWS) if needed during induction; collect/run urine drug screen (UDS); check Prescription Drug Monitoring Plan (PDMP)
Primary Care Provider
- Confirm DSM-5 diagnosis, assess comorbid conditions, monitor progress
Clinic medical director
- Ensure protocols in place and appropriate billing
Counselor (if available - absence shouldn’t prevent starting OBOT)
- Behavioral counseling, monitoring
Essential Training for Clinic Team Goal: Develop Shared Philosophy and Scope
Recognizing and monitoring withdrawal symptoms (vs. “acting out”)
Importance of timely buprenorphine refills (vs. “we’ll let the provider know…”)
Embrace substance use disorder as medical condition (vs. moral failure)
Urine drug screening as medical safety (vs. policing activity)
Timing of buprenorphine induction
Relapse is common and does not equal failure
- Goal is to limit duration and build on success
Timing of Buprenorphine Induction
Schedule patient for induction soon after intake visit
- Or provider education on home induction
Must be in at least mild-to-moderate opioid withdrawal in order to begin induction
- The more severe the withdrawal, the greater the relief
Withdrawal symptoms typically begin
- 12-24 hours after last dose of a short-acting opioids like heroin
- 2-4 days after last dose of long acting opioids like methadone
Clinical Opioid Withdrawal Scale (COWS)
Measures withdrawal symptoms
Guides timing of first dose of buprenorphine
Easily administered by medical assistants and nurses
COWS Assessment Rates 11 Withdrawal Symptoms:
Resting pulse rate
Sweating
Restlessness
Pupil size
Bone or joint aches
Runny nose
GI upset
Tremor
Yawning
Anxiety or irritability
Goose bumps
Buprenorphine/Naloxone Treatment Phases
Induction (1-3 days)
−Must be in moderate withdrawal
−Start with 4mg and gradually increase
−Titrate to effect (average dose 16mg)
Stabilization/Maintenance
- Combine with random UDS and counseling, if available
- Lack of counseling shouldn’t prevent treatment
- Provider medical management as “counseling”
- Patients typically continue buprenorphine for years
|
Typical Buprenorphine Clinic Schedule
A Rough Guide to Tailor to Practice and Patient
|
|
Before
Induction
|
Induction’
(Days 1-3)
|
Month 1
|
Month 2
|
Month
|
|
Prior Authorization
|
X
|
|
|
|
|
|
Treatment Agreement
|
X
|
|
|
|
|
|
Clinic Visit
|
X
|
2x/week
|
Weekly
|
Every 2 weeks
|
Every 4 weeks
|
|
Counseling
|
X
|
|
Weekly
|
Every 2 weeks
|
Every 4 weeks
|
|
Refill
|
|
1-3 day supply
|
7 day supply
|
14 day supply
|
28 day supply
|
|
|
Recommended Staff of Offices Providing MAT*
1. DATA 2000-waivered physicians, nurse practitioners, and physician assistants
2. Nurses: registered nurses, nurse care managers
3. Behavioral health: social workers, counselors, psychologists and substance use disorder counselors
4. Clinicians who can practice in an integrated model, addressing both primary care and behavioral health issues
* National Association of Community Health Centers. (2018). Business plan for medication assisted training. Providers Clinical Support System (PCSS) at: https://pcssnow.org/resource/business-plan-for-medication-assisted-treatment-mat/
|
|
|
The WRAP App – A Recovery Tool for Patients with OUD
What is WRAP?
The Wellness Recovery Action Plan or WRAP, is a self-designed prevention and wellness process that anyone can use to get well, stay well and make their life the way they want it to be. It was developed in 1997 by a group of people who were searching for ways to overcome their own mental health issues and move on to fulfilling their life dreams and goals. It is now used extensively by people in all kinds of circumstances, and by health care and mental health systems all over the world to address all kinds of physical, mental health and life issues.
Overview of the WRAP App
- Clients discover their own simple, safe wellness tools
- Clients develop for themselves a list of things to do every day to stay as well as possible
- Clients identify upsetting events, early warning signs and signs that things have gotten much worse and, commit to using wellness tools, develop action plans for responding at these times
- Clients create their own unique crisis plans
- Clients create their own post-crisis plan
What OUD Patients gain from using the WRAP App
They can use this simple and powerful process on the App for creating the life and wellness they want. They can:
- Shape every aspect of their life the way they want it to be
- Gain freedom from troubling thoughts, behaviors, or patterns that repeat in their life
With the WRAP App they can:
- Discover simple, safe, and effective tools to maintain wellness
- Develop a daily plan to stay on track with their life goals
- Identify what throws them off track and develop a plan to keep moving forward
- Gain support and stay in control even in a crisis
How to get the WRAP App
You can download the WRAP App
From the Apple store at: https://apps.apple.com/us/app/wellness-recovery-action-plan/id1450222981?ls=1
From the Google Android store at: https://play.google.com/store/apps/details?id=com.ahpnet.wrap&hl=en_US
Websites with more information on WRAP are:
WRAP Wellness Recovery Action Plan at: https://mentalhealthrecovery.com/wrap-is/
Copeland Center for Wellness and Recovery- What is WRAP at: https://copelandcenter.com/wellness-recovery-action-plan-wrap
|
|
|
Benefits of Office-Based MAT Treatment*
• Improved access
• Private, confidential, and safe treatment that can be provided in any physician’s office or health center
• Allows for continuity of care with primary provider including supervision of any controlled substances
• Does not require daily visits to a clinic or out-of-town, costly residential treatment
• May allow more patient time for work, family, and other activities
• Close supervision and regular use of clinic services for monitoring and diversion
*National Association of Community Health Centers. (2018). Business plan for medication assisted training. Providers Clinical Support System (PCSS) at: https://pcssnow.org/resource/business-plan-for-medication-assisted-treatment-mat/
|
|
Hub - and – Spoke of MAT Medical Practice
Pharmacologic:
Primarily buprenorphine-naloxone
Coordination/Integration of Care:
Coordination and integration between hub and spoke as well as within each spoke
RN case manager and/or care connector (peer or behavioral health specialist) organizes care coordination
Education/Outreach:
Outreach to community prescribers to increase pool of providers with buprenorphine prescribing waivers
Psychosocial:
Embedded within spoke site Includes social workers, counselors, community health teams
Other:
Hub provides consultation services - Available to manage clinically complex patients, MAT tapering, methadone prescribing
Funding: CMS State Medicaid waiver
Buprenorphine/Naloxone: Decreased Diversion Potential
Precipitated withdrawal when injected
When diverted, mostly used for self-treatment of withdrawal, instead of intoxication
Low overdose risk decreases possibility of harm if diverted
Strategies to Limit Diversion
Caution when prescribing
- Use lowest dose that works
Urine toxicology screens
PDMP queries (Prescription Drug Monitoring Program)
Pill Counts
Long-acting preparations
- Monthly XR-naltrexone depot injection
- Monthly buprenorphine depot injection
- 6-Month buprenorphine implant (stable patients)
Criteria Used to Determine Level of Care
The degree of severity within 6 Dimensions determines the level of care:
1.Substance Intoxication and Withdrawal Potential
2.Medical Conditions and Complications (e.g., seizures)
3.Emotional/Behavioral/Psychiatric Conditions (e.g., depression, anxiety)
4.Readiness to Change (e.g., motivation)
5.Relapse/Continued Use/Continued Problem (e.g., DSM-5) Potential
6.Recovery Environment (How much social support does the client have
Standard Medical Management (SMM) for Opioid Use Disorder (OUD)
1. The Goals of SMM
- Abstinence and Opioid Use Disorder Remission
- Reduction of use and problesm
2. The Elements of SMM
- Provision of buprenorphine induction and/or maintenance
- Education regarding OUD and buprenorphine treatment
- Monitoring of compliance with buprenorphine
- Monitoring of patients’ drug use, symptoms, and progress
- Encouragement for abstinence and treatment adherence
- Encouragement for mutual-support groups and/or self-help
- Motivational enhancement
- Brief advice modeled on standard drug counseling
- Treatment of medical complications of opioid use
- Referrals to specialty services in the community
3. The Roles of SMM
Physician (PA or APRN): ALL elements of SMM; supervision of nurse
- Meets w/ patient for initial and subsequent monthly appointments
Nurse: All elements of SMM, EXCEPT prescribing of buprenorphine
Counselors: Only the psychosocial components of SMM when an RN is not available.
4. The Sequence of SMM
- Initial session 45-60 minutes
- Subsequent sessions 15-20 minutes
Initial SMM Session: 45-60 mins
Establish rapport with the patient
Review medical, psychiatric and substance use and treatment history
Quickly review who they are aside from their substances (place of birth, education, employment, family supports)
Review diagnosis of OUD with the patient
Develop the treatment plan (including buprenorphine)
Advise abstinence from all drugs
Refer to mutual-support group
Motivational Enhancement
Other referrals
Delineate and reinforce the program guidelines
Answer any questions the patient may have
Foundation Skills in SMM Sessions
Reflective Listening
Open-Ended Questions
Establish Rapport: Introduce; Explain, Ask Permission
Review Problems: Ask, Reflect, Give Information
Review Diagnosis: Review DSM-5 Diagnosis; Provide Evidence, Summarize
Develop Treatment Plan: Treatable, Rationale for Suboxone and Counseling
Provide Advice: Abstinence, SMM Adherence, Mutual Support Groups
Standard Drug Counseling and Triggers (RACE)
- Recognize Triggers as early as possible
- Avoid triggers as much as possible
- Cope differently with triggers that cannot be avoided
- Escape from triggering situations when avoidance and/or coping strategies are beginning to fail
Other Counseling Approaches to be used along with SMM
MBSR Mindfulness Based Stress Reduction Training (especially for Pain relate OUD)
Motivational Interviewing (MI)
Cognitive-Behavioral Therapy (CBT)
Individual and Group Drug Counseling (DC)
Community Reinforcement Approach (CRA)
Contingency Management (CM)
Twelve-Step Facilitation (TSF)
Cognitive Therapy (CT)
|
Standard Medical Management Outline
|
GENERAL
|
Empathic, Hopeful Positive
|
“We can effectively manage this.”
|
|
Initial Session
|
Rapport
Problems
Diagnosis
Rx Plan
Advice and Referrals
Guidelines
Questions
|
“What are your goals, here?”
“What troubles you about your use?”
“Based on our assessment, you have an OUD…”
“We recommend daily buprenorphine and weekly visits for counseling.”
“We strongly suggest abstinence.”
“We have some information about housing for you.”
“Our program’s expectations of you are…”
“Please feel free to ask any questions [PAUSE]…”
|
|
Follow Up Sessions
|
Compliance
Response
Changes
Advice
New referrals
Medication
|
“Tell me about times you missed your buprenorphine.”
“How do you think it’s working?” (Check utox results also)
“How’s it gone with cravings, use and avoidance of triggers?”
“We recommend that you stay away from friends who use.”
“I’d also like to refer you to a new job program.”
“Here’s your new prescription.”
|
|
FAQs
|
Open Questions Reflections
Advice
|
"Tell me more about that? Is there a “flip-side?”
“Sounds like you’re saying…”
“Given all of this, I suggest you…”
“How ready do you feel to do that?”
“What might be some of your reasons?”
“What’s your next step, if any?”
|
Regulation of Medication Assisted Treatment of OUD
Drug Addiction Treatment Act of 2000 (DATA 2000)
- An amendment to the Controlled Substances Act
- Allows practitioner to prescribe FDA approved narcotic drugs in schedule III, IV, V, or combinations of such drugs, for maintenance or detoxification treatment
- Permits no limitations on the quantities of the drugs that may be provided for unsupervised use, unless the drugs have been subject to adverse determination
- Drugs and practitioner must meet certain requirements
Practitioner Requirements:
- “Qualifying physician”
- Has capacity to refer patients for appropriate counseling and ancillary services
- No more than 30 patients (individual practice) for the first year
- May request approval to treat up to 100 patients after the first year
- Board certified in Addiction Psychiatry
- Certified in Addiction Medicine by the American Board of Addiction Medicine (ABAM)
- Certified in Addiction Medicine by the American Osteopathic Academy (AOA)
- Investigator in buprenorphine clinical trials leading to FDA approval
- Has completed 8 hours of training provided by one of the following organizations (or others designated by HHS):
- Providers Clinical Support System (PCSS) MAT Training
- American Academy of Addiction Psychiatry (AAAP)
- American Medical Association (AMA)
- American Osteopathic Academy of Addiction Medicine (AOAAM)
- American Psychiatric Association (APA)
- American Society of Addiction Medicine (ASAM)
- Training/experience as determined by state medical licensing board
- Other criteria established by the Secretary of HHS
Must notify the Secretary of HHS online:
- His/Her name
- DEA registration
- Category for qualification
- Certify intention to comply with law
Notifications must be submitted online at:
http://buprenorphine.samhsa.gov/forms/select-practitioner-type.php
Narcotic Drug according to DATA 2000
(Narcotic is used here in the legal sense of the Controlled Substances Act: It includes all opioid products as well as other drugs and medications such as cocaine and illegal substances)
- Approved by the FDA for use in maintenance or detoxification treatment of opioid use disorder
- Schedule III, IV, or V
- Drugs or combinations of drugs
- Buprenorphine is the only drug currently approved (Schedule III)
|
Buprenorphine Formulations - DATA 2000
|
CARA 2016 Legislation: Signed into law 7/22/2016
Revised Regulations:
- Physicians may request approval to treat up to 275 patients after one year at 100 patients (as allowed under DATA 2000)
- These physicians must be board certified in addiction psychiatry or addiction medicine or practice in a qualified practice setting
- Annual reporting requirements
- Expands prescribing privileges to nurse practitioners (NPs) and physician assistants (PAs) for five years (until October 1, 2021)
- NPs and PAs must complete 24 hours of training to be eligible for a waiver to prescribe and must be supervised by or work in collaboration with a qualifying physician if required by state law
Qualified Practice Setting:
- Provides 24 hour emergency coverage
- Provides case management and related services
- Use health information technology
- Registered with state prescription monitoring program
- Accepts third-party payment for some services
New Standards of Care:
- Board certified practitioners
- Access to behavioral health services
- Follows evidence-based treatment guidelines
- Individualized treatment plans
- Diversion control plans
- Use of state Prescription Drug Monitoring Program (PDMP)
- Annual reporting requirements
CARA Reporting Requirements
- Average monthly caseload of patients receiving buprenorphine based MAT, per year
- Percentage of patients who had a Prescription Drug Monitoring Program (PDMP) query in the past month
- Percentage of active buprenorphine patients that received psychosocial services (either by direct provision, including medical management or referral) in the past year due to:
- Treatment initiation
- Change in clinical status
|
Doctors with the Waiver to Administer Suboxone in Tampa Bay Area
To assist you find doctors who administer Suboxone, we collated the names and addresses and telephone numbers of Doctors' offices in Hillsborough, Pasco, and Pinellas County. Download the document below for this information.
|
|
|