Unit 1: Overview of Motivational Interviewing
|
|
Motivational Interviewing - A Training Resource
By Jim Messina
|
|
|
A Helping Truism:
How many helpers does it take to change a light bulb?
Just one, but the light bulb has to want to be changed.
|
What is Motivational Interviewing
Motivational Interviewing (MI) is a client-centered method for helping people explore and resolve their ambivalence to change. Treatment providers using MI express empathy, develop discrepancy, roll with resistance, and support self-efficacy. The definition of Motivational (MI) has evolved and been refined since the original publications on its utility as an approach to behavior change.
Treatment providers using MI express empathy, develop discrepancy, roll with resistance, and support self-efficacy. The definition of Motivational (MI) has evolved and been refined since the original publications on its utility as an approach to behavior change. The initial description, by Stephen Rollnick and William R. Miller in 1983, developed from their experience in the treatment of problem drinkers (Miller & Rollnick, 2013). Through clinical experience and empirical research, the fundamental principles and methodologies of MI have been applied and tested in various settings (Substance Use Disorder Treatment Centers, Primary Medical Centers, Schools, Probation Offices and others) and research findings have demonstrated its efficacy. MI is now established as an evidence based practice in the treatment of individuals with substance use and addictive disorders (gambling, smoking, alcohol and drugs) and a variety of medical conditions (obesity, diabetes, asthma, chronic pain, increase of physical exercise etc.).
|
Miller and Rollnick’s Three Definitions of Motivational Interviewing (2013)
Layperson’s definition: Motivational interviewing is a collaborative conversation style for strengthening a person’s own motivation and commitment to change.
Practitioner’s definition: Motivational interviewing is a person-centered counseling style for addressing the common problem of ambivalence about change.
Technical definition: Motivational interviewing is a collaborative, goal-oriented style of communication with particular attention to the language of change. It is designed to strengthen personal motivation for and commitment to a specific goal by eliciting and exploring the person’s own reasons for change within an atmosphere of acceptance and compassion.
|
Motivational Interviewing focuses on exploring and resolving ambivalence and centers on motivational processes within the individual that facilitate change. MI differs from more “coercive” or externally driven methods for motivating change as it does not impose change (that may be inconsistent with the person's own values, beliefs or wishes); but rather supports change in a manner congruent with the person's own values and concerns.
|
Source for Materials on Motivational Interviewing:
Miller, W.R. & Rollnick, S. (2013). Motivational interviewing: Helping people change (Applications of motivational interviewing), 3rd edition. New York: Guilford Press.
Rollnick, S., Miller, W.R., & Butler, C.C. (2008). Motivational interviewing in Health Care: Helping Patients Change Behavior. New York: Guilford Press.
|
The Guiding Principles of Motivational Interviewing
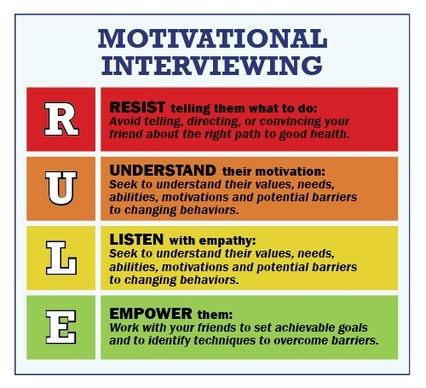
The practice of MI has four guiding principles: (1) to resist the righting reflex, (2) to understand and explore the clients’ own motivations, (3) to listen with empathy, and (4) to empower the clients, encouraging hope and optimism. These four principles fit the acronym RULE: Resist, Understand, Listen, and Empower (Rollnick, Miller, & Butler, 2008).
R: Resist the Righting Reflex with Clients
People who enter helping professions often have a powerful desire to set things right, to heal, to prevent harm and promote well-being which is called the Righting Reflex. When seeing someone headed down the wrong path, helpers will usually want to get out in front of the person and say, “Stop! Turn back! There is a better way!” Given this motivation, the urge to correct another’s course often becomes automatic, almost reflexive. A problem is that this first inclination can have a paradoxical effect. The reason is not that clients are flawed, recalcitrant, lazy, or in the denial. Rather, it is a natural human tendency to resist persuasion. This is particularly true when one is ambivalent about something. Problem drinkers, for example, often know perfectly well that they are drinking too much and that it is having some adverse consequences. But they also enjoy drinking and don’t like to think of themselves as “having a problem,” and thus they prefer to see their drinking as reasonably normal.
U: Understand the Clients’ Motivations
It is the clients’ own reasons for change, and not the helpers that are most likely to trigger behavior change. And so helpers need to be interested in the clients’ own concerns, values, and motivations. In MI helpers proceed in a way that evokes and explores clients’ perceptions about their current situations and their own motivations for change.
|
L: Listen to the Clients
MI involves at least as much listening as informing. Perhaps the normal expectations of a professional consultation are that the helpers have the answers and will give them to their clients. Often helpers do have answers, and clients come to them for this expertise. When it comes to behavior change, though, the answers most likely lie within the clients and finding them requires some listening. Good listening is actually a complex clinical skill. It requires more than asking questions and keeping quiet long though to hear clients’ replies.
|
E: Empower the Client
It is increasingly clear that outcomes are better when clients take an active interest and role in their own health care. Empowerment is helping clients explore how they can make a difference in their own health. Again, the clients’ own ideas and resources are key here. Helpers know that regular exercise is important, but it is their clients who know best how they could successfully build it into their daily lives. Clients in MI become the helpers’ consultants on their own lives and on how best to accomplish behavior change. An important role for the helpers in this process is to support their hope that such change is possible and can make a difference in their health. Clients who are active in the consultation, thinking aloud about the why and how of change, are more likely to do something about this afterward.
|
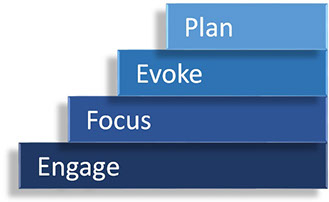
Four Processes in Motivational Interviewing (Miller & Rollnick, 2013)
1. Engaging: is the process by which both parties establish a helpful connection and a working relationship. Therapeutic engagement is a prerequisite for everything that follows and it involves developing a working alliance.
2. Focusing: is the process by which helpers and clients develop and maintain a specific direction in the conversation about change. In the course of helping relationships, a direction towards one or more change goals usually emerges.
3. Evoking: involves eliciting the clients’ own motivations for change, and it has always been at the heart of MI. It occurs when there is a focus on a particular change and the providers harness the clients’ own ideas and feelings about why and how they might do it. Evoking is having the clients voice the arguments for change.
4. Planning: encompasses both developing commitment to change and formulating a specific plan of action. It’s a conversation about action that can cover a range of topics, conducted with a sharp ear for eliciting clients’ own solutions, promoting their autonomy of decision making and continuing to elicit and strengthen change talk as a plan emerges.
|
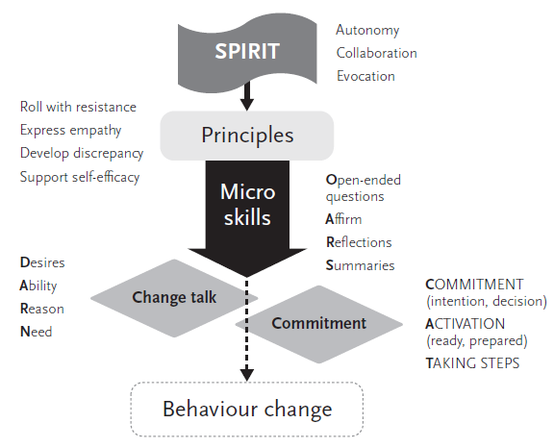
The Spirit of Motivational Interviewing (Miller & Rollnick, 2013)
1. Collaboration (vs. Confrontation)
Collaboration is a partnership between the helper and the clients, grounded in the point of view and experiences of the clients. This contrasts with some other approaches which are based on the helpers assuming an “expert” role, at times confronting the clients and imposing their perspective on the clients’ problem behaviors and the appropriate course of treatment and outcome. Collaboration builds rapport and facilitates trust in the helping relationship, which can be challenging in a more hierarchical relationship. This does not mean that the helpers automatically agree with the clients about the nature of the problem or the changes that may be most appropriate. Although they may see things differently, the therapeutic process is focused on mutual understanding, not the helper being right.
2. Evocation (Drawing Out, Rather Than Imposing Ideas)
The MI approach is one of the helpers’ drawing out the individuals' own thoughts and ideas, rather than imposing their opinions as motivation and commitment to change is most powerful and durable when it comes from the clients. No matter what reasons the helpers might offer to convince the clients of the need to change their behavior or how much they might want them to do so, lasting change is more likely to occur when the clients discover their own reasons and determination to change. The helpers’ job is to "draw out" the persons' own motivations and skills for change, not to tell them what to do or why they should do it.
|
3. Autonomy (vs. Authority)
Unlike some other treatment models that emphasize the clinicians/helpers as authority figures, Motivational Interviewing recognizes that the true power for change rests within the clients. Ultimately, it is up to the individuals to follow through with making changes happen. This is empowering to the individuals, but also gives them responsibility for their actions. Helpers reinforce that there is no single “right way” to change and that there are multiple ways that change can occur. In addition to deciding whether they will make a change, clients are encouraged to take the lead in developing a “menu of options’ as to how to achieve the desired change.
4. Compassion
The interviewers act benevolently to promote the clients’ welfare, giving priority to the clients’ needs. Interviewers are for their clients benefit and not primarily for their own. Compassion is a deliberate commitment to pursue the welfare and best interests of others. It is this promotion of others’ welfare which motivates people to be drawn to the helping professions. To work with a spirit of compassion is interviewers’ having their hearts in the right place so that the trust they engender will be deserved
|
The Principles of Motivational Interviewing (Miller & Rollnick, 2013)
Building on and bringing to life the elements of the MI “style”, there are four distinct principles that guide the practice of MI. The helpers employing MI will hold true to these principles throughout treatment.
Principle 1: Express Empathy
- Expressing empathy towards the clients shows acceptance and increases the chance of developing a rapport.
- Acceptance enhances self-esteem and facilitates change.
- Skillful reflective listening is fundamental.
- Clients’ ambivalence is normal.
|
Principle 2: Develop Discrepancy
- Developing discrepancy enables the clients to see that their present situation does not necessarily fit into their values and what they would like in the future.
- The clients rather than the helpers should present the arguments for change.
- Change is motivated by a perceived discrepancy between present behavior and important personal goals and values.
|
Principle 3: Roll with Resistance
- Rolling with resistance prevents a breakdown in communication between clients and helpers and allows the clients to explore their views.
- Avoid arguing for change.
- Do not directly oppose resistance.
- New perspectives are offered but not imposed.
- The clients are a primary resource in finding answers and solutions.
- Resistance is a signal for the helpers to respond differently.
Motivational Interviewing is like Dancing with the Clients not Wrestling with the Clients- So roll with the Resistance.
|
Principle 4: Support Self-efficacy
- Self-efficacy is a crucial component to facilitating change. If the clients believe that they have the ability to change, the likelihood of change occurring is greatly increased.
- Clients’ beliefs in the possibility of change is an important motivator.
- The clients, not the helpers, are responsible for choosing and carrying out change.
- The helpers’ believe in the clients’ ability to change becomes a self-fulfilling prophecy.
|
Motivational Interviewing Skills and Strategies (Miller & Rollnick, 2013)
The practice of Motivational Interviewing involves the skillful use of certain techniques for bringing to life the “MI spirit”, demonstrating the MI principles, and guiding the process toward eliciting clients’ change talk and commitment for change. Change talk involves statements or non-verbal communications indicating the clients may be considering the possibility of change.
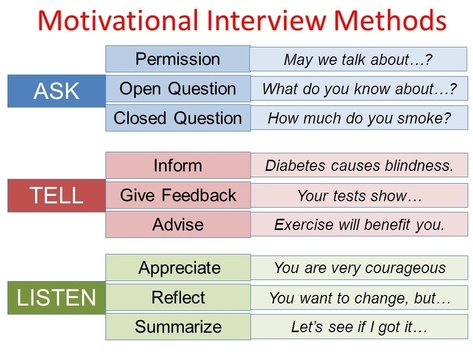
OARS
OARS is a mnemonic to remember the basic approach used in Motivational Interviewing. Open Ended Questions, Affirmations, Reflections, and Summaries are core counselor behaviors employed to move the process forward by establishing a therapeutic alliance and eliciting discussion about change.
O - Open-ended questions are those that are not easily answered with a "yes/no" or short answer containing only a specific, limited piece of information. Open-ended questions invite elaboration and thinking more deeply about an issue. Although closed questions have their place and are at times valuable (e.g., when collecting specific information in an assessment), open-ended questions create forward momentum used to help the clients explore the reasons for and possibility of change.
|
A - Affirmations are statements that recognize clients’ strengths. They assist in building rapport and in helping the clients see themselves in a different, more positive light. To be effective they must be congruent and genuine. The use of affirmations can help clients feel that change is possible even when previous efforts have been unsuccessful. Affirmations often involve reframing behaviors or concerns as evidence of positive clients’ qualities. Affirmations are a key element in facilitating the MI principle of Supporting Self-efficacy.
R - Reflections or reflective listening is perhaps the most crucial skill in Motivational Interviewing. It has two primary purposes. First is to bring to life the principle of Expressing Empathy. By careful listening and reflective responses, the clients come to feel that the helpers understand the issues from their perspective. Beyond this, strategic use of reflective listening is a core intervention toward guiding the clients toward change, supporting the goal‐directed aspect of MI. In this use of reflections, the helpers guide the clients towards resolving ambivalence by a focus on the negative aspects of the status quo and the positives of making change. There are several levels of reflection ranging from simple to more complex. Different types of reflections are skillfully used as clients demonstrate different levels of readiness for change. For example, some types of reflections are more helpful when the clients seem resistant and others more appropriate when the clients offer statements more indicative of commitment to change.
S - Summaries are a special type of reflection where the helpers recaps what has occurred in all or part of a counseling session(s). Summaries communicate interest, understanding and call attention to important elements of the discussion. They may be used to shift attention or direction and prepare the clients to “move on.” Summaries can highlight both sides of clients’ ambivalence about change and promote the development of discrepancy by strategically selecting what information
|
Change Talk (Miller & Rollnick, 2013)
Change talk is defined as statements by the clients revealing consideration of, motivation for, or commitment to change. In Motivational Interviewing, the helpers seek to guide the clients to expressions of change talk as the pathway to change. Research indicates a clear correlation between clients’ statements about change and outcomes-client-reported levels of success in changing a behavior. The more clients talk about change, the more likely they are to change. Different types of change talk can be described using the mnemonic DARN-CAT.
Preparatory Change Talk
D - Desire (I want to change)
A - Ability (I can change)
R - Reason (It’s important to change)
N - Need (I should change)
And most predictive of positive outcome:
Implementing Change Talk
C - Commitment (I will make changes)
A - Activation (I am ready, prepared, willing to change)
T - Taking Steps (I am taking specific actions to change)
|
Strategies for Evoking Change Talk (Miller & Rollnick, 2013)
There are specific therapeutic strategies that are likely to elicit and support change talk in Motivational Interviewing:
1. Ask Evocative Questions: Ask an open question, the answer to which is likely to be change talk.
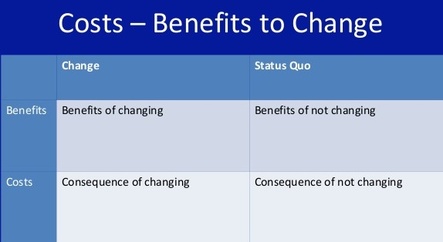
2. Explore Decisional Balance: Ask first for the good things about status quo, then ask for the not-so-good things.
3. Ask for Elaboration: When a change talk theme emerges, ask for more details. In what ways? Tell me more…? What does that look like?
4. Ask for Examples: When a change talk theme emerges, ask for specific examples.
When was the last time that happened? Give me an example. What else?
5. Look Back: Ask about a time before the target behavior emerged. How were things better, different?
6. Look Forward: Ask what may happen if things continue as they are (status quo). Try the miracle question: If you were 100% successful in making the changes you want, what would be different? How would you like your life to be five years from now?
7. Query Extremes: What are the worst things that might happen if you don’t make this change? What are the best things that might happen if you do make this change?
8. Use Change Rulers: Ask: “On a scale from 1 to 10, how important is it to you to change (the specific target behavior) where 1 is not at all important, and a 10 is extremely important? Follow up: “And why are you at ___ and not ____ (a lower number than stated)?” “What might happen that could move you from _____to ____ (a higher number)?” Alternatively, you could also ask “How confident are that you could make the change if you decided to do it?”
|
NOTE: Instead of “how important” (need), you could also ask how much you want (desire), or how confident you are that you could (ability), or how committed are you to (commitment). Asking “how ready are you?” tends to be confusing because it combines competing components of desire, ability, reasons and need.
9. Explore Goals and Values: Ask what the clients’ guiding values are. What do they want in life? Ask how the continuation of target behavior fits in with the clients’ goals or values. Does it help realize an important goal or value, interfere with it, or is it irrelevant?
10. Come Alongside: Explicitly side with the negative (status quo) side of ambivalence. “Perhaps ____is so important to you that you won’t give it up, no matter what the cost.”
|
Change Talk vs Sustain Talk (Miller & Rollnick, 2013)
What is Sustain Talk? Sustain Talk is when clients talk about their favoring their "status quo" rather than movement toward "change goals."
What is Change Talk? Change Talk is when clients talk about their favoiring movement towards "change goals."
|
What is Discord?
It is the interpersonal behavior in the MI process that reflects dissonance in the working relationship between the helpers and clients. Sustain talk in itself does not constitute discord. What follows are the examples of discord:
Discord in MI has various elements
- Arguing: Clients contest the accuracy, expertise, or integrity of the helpers
- Interrupting: Clients break in and interrupts the helpers in a defensive manner
- Discounting: Clients express unwillingness to recognize problems, cooperate, accept responsibility, or take advice
- Ignoring: Clients show evidence of ignoring or not following the helpers
What skills are needed to respond to either Sustain Talk or Discord so as to get back to Change Talk
- Simple Reflection: The simplest approach to responding to resistance is with nonresistance, by repeating the clients' statements in a neutral form. This acknowledges and validates what the clients have said and can elicit an opposite response.
- Shifting Focus: Helpers can defuse resistance by helping the clients shift focus away from obstacles and barriers. This method offers an opportunity to affirm the clients' personal choices regarding the conduct of their own lives.
- Reframing: This is good strategy to use when clients deny personal by offering a new and positive interpretation of negative information provided by the clients. Reframing acknowledges the validity of the clients' raw observations, but offers a new meaning.
- Rolling with the Resistance: Momentum can be used to good advantage and perceptions can be shifted. New perspectives are invited but not imposed.The clients are a valuable resource in finding solutions to problems
- Develop Discrepancy: Motivation for change is enhanced when clients perceive differences between their current situation and their hopes for the future. Developing awareness of consequences helps clients examine their behaviors. A discrepancy between present behaviors and important goals motivates change. The clients should present the arguments for change.
|
The Framework of Motivational Interviewing
|
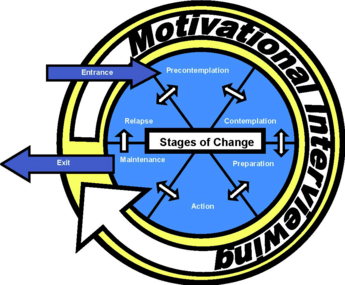
The Stages of Change in the
Transtheoretical Model (TTM) of Change
Prochaska and DiClemente (1983)
Stages of TTM of Change Model
- Pre-contemplation
- Contemplation
- Preparation
- Action
- Maintenance
1. Pre-contemplation
Task - to increase discrepancy
Educational confrontation - How many joints do you smoke?
Use progression models
Accurate information about disease
Educational model
Good and less good aspects
Invites defensiveness
Narcissistic defense
Broad based assessment
Alcohol and drug history
Psychosocial history
Psychiatric evaluation
Medical evaluation
|
2. Contemplation
Task - tip the decisional balance scale
Normalize ambivalence
I know many other clients who felt the same way as you and they succeeded.
You are the best judge of which way to go.
Use reframing
What are the options?
Move from external to internal motivation
Real from perceived
There are many problems
Deal with first other issue
“Natural link”
Quit drinking for a week
Take meds for a month
List of concerns
“Pro’s and con’s”
Questions
It’s up to you…….
What do you plan to do next?
What is most important reason to change?
Where do we go from here?
How would you like for things to turn out?
|
3. Preparation
Identify and assist in problem solving re: obstacles
Help client identify social support
Verify that client has underlying skills for behavior change
Encourage small initial steps
4. Action
Practicing new behaviors
Focus on restructuring cues and social support
Bolster self-efficacy for dealing with obstacles
Combat feelings of loss and reiterate long-term benefits
|
5. Maintenance
Continued commitment to sustaining new behavior
Plan for follow-up support
Reinforce internal rewards
Discuss coping with relapse
Prochaska, J.Q. & DiClemente, C.C. (1983). Stages and processes of self-change of smoking: Toward an integrative model of change. Journal of Consulting and Clinical Psychology, 51(3), 390-395.
|
TTM defines stages of change and
Motivational Interviewing provides a means of moving through the stages
|
Clearing the Air about Misconceptions about Motivational Interviewing
|
MI is Not:
|
MI is:
|
|
1. Identical to Rogers’ non-directive counseling
|
1. MI’s focusing, evoking, and planning have clear directionality to them.
|
|
2. A technique or gimmick to make people change
|
2. MI was specifically developed to help clients resolve ambivalence and strengthen their own commitment to change
|
|
3. MI is a panacea, the solution to all clinical problems
|
3. MI blends well with other approaches and does not negate the value of other techniques. MI is a style of being with people, an integration of clinical skills to foster movement for change.
|
|
4. The Transtheoretical Model (TTM) of Change, although they are compatible and complementary.
|
4. TTM defines stages of change while MI provides a means of moving through the stages
|
|
5. The “Decisional Balance” technique exploring the pros and cons of change
|
5. Decisional balance is more associated with counseling with neutrality as the counselor explores con’s of change. MI is more directional, with the intent being to strengthen the arguments for change
|
|
6. Require the use of assessment feedback
|
6. While personal feedback may be particularly useful for persons who aren’t considering change, it is not a necessary nor a sufficient component of MI.
|
|
7. A way of manipulating people into doing what you want them to do
|
7. MI cannot be used to manufacture motivation that isn’t already there. It is a collaborative partnership that honors and respects the other’s autonomy, seeking to understand the person’s internal frame of reference.
|
|
Learning Motivational Interviewing
12 Steps to Leaning Motivational Interviewing (Miller & Rollnick,
2013)
1.
Understanding the underlying MI Spirit
2.
Developing skill and comfort with reflective listening
3. Identifying
change goals (Focusing)
4.
Exchanging information and providing advice within an MI style (Engaging, Planning,
Evoking)
5. Being
able to recognize Change Talk and Sustain Talk
6.
Evoking Change Talk
7.
Responding to Change Talk in a manner that strengthens it
8.
Responding to Sustain Talk and Discord in a way that does not amplify it
9.
Developing hope and confidence
10.
Timing and negotiating a change plan
11.
Strengthening commitment
12.
Flexibly integrating MI with other clinical skills and practices
|
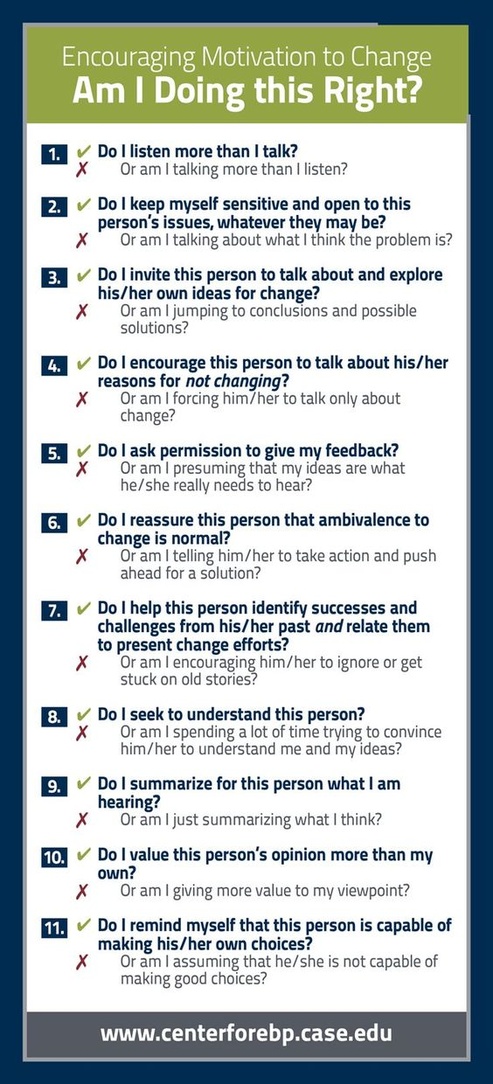
How can the 12 learning tasks be accomplished? (Miller &
Rollnick, 2013)
More than
obtaining knowledge is involved. Feedback is fundamental and the more immediate
the better “it’s hard to learn archery in the dark.” Clients provide immediate
feedback through their responses to the helper.
Developing Proficiency in MI
What’s
needed? Knowledge development and the opportunity for continued learning over
time through feedback and coaching based on direct observation. However, coaching
need not be extensive. It is a matter of learning and applying the MI criterion
which is important and not completing a fixed number of training hours which
makes for competent MI helpers.
Personal Tip for Improving your MI Skills
Listening
to your own sessions by recording them (with permission) your session and then:
- Count your reflections: were they simple or complex? Offer
more complex than simple reflections
- Count your questions: were they open or closed? Ask
more open than closed questions
- Count both reflections and questions: what is your
ratio? Aim for 2 reflections for every question
- Listen for Change Talk and Sustain Talk: count each
and determine the ratio. Equal frequency = ambivalence (no change) - When
Change Talk occurred, what was the next thing you said? Count your OARS
responses
- Listen for MI inconsistent responses (giving advice
without permission, confronting or arguing with the client, other
“righting reflex” responses - How did the client respond to these?
|
Stephen Rollnick’s 5 Steps to Help Trainees in Learning Motivational Interviewing - Unlearn
- Slow Down
- Be humble
- Believe in them
- Go with their language about change
Final Note on Training Workshop training is a good start but it is just the beginning. Feedback and coaching are important in learning MI and need to be based on observed practice and continued over time, even for the experts. Skills tend to drift over time. Skill development in MI is not a one-shot event but an ongoing process. Best of Luck!
|
|
|