Unit 1: Assessment of Suicidal Ideation, Intent and Behavior
|
|
Suicide Intervention and Prevention Strategies - A Training Resource
|
|
|
Myths and FACTS About Suicide
Myth: Most people who die by suicide don’t make future plans
FACT: The suicidal mind is characterized by ambivalence. People make plans for their jobs, trips and relationship in the days and weeks leading up to their suicides.
Myth: Suicide is selfish, a reflection of excessive self-focus.
FACT: It is Important to distinguish aborted attempts from actual attempts and suicide and one must rule psychopaths from the persons with aborted attempts
Myth: Suicide is an easy escape, one that cowards use.
FACT: In clinical case studies of Holocaust victims/survivors it was found that often the self-preservation instinct resulting in “Hesitation” wounds
Myth: A person who talks about suicide won’t really follow through.
FACT: Eight out of 10 people who commit suicide have spoken about their intent before killing themselves.
Myth: Only insane people commit suicide.
FACT: People who commit suicide may feel hopeless and depressed, but have not necessarily lost touch with reality. Suicide is 4 times more likely for depressed people.
Myth: Talking about suicide might prompt the person to act.
FACT: Discussing the subject openly shows that you take the person seriously and that you care. It’s helpful, not harmful.
Myth: Suicide is a problem among old people – not young people.
FACT: Suicide is a problem among the elderly. But the suicide rate among 15-24-year-olds has tripled in the past 30 years.
Myth: No one I know is the type to commit suicide.
FACT: Suicide occurs among young people of ALL types – rich and poor, athletic and non-athletic, popular and unpopular, etc.
Myth: People who attempt suicide are just trying to get attention.
FACT: Possibly, but unless someone gives them some appropriate attention, the results could be fatal.
Myth: Once a person decides to commit suicide, nothing can stop that person.
FACT: On the contrary, most people want to be stopped from taking their lives. (But remember – not everyone can be stopped, though the effort of trying may save a life.)
Myth: People who attempt suicide really want to die.
FACT: Most people want to end their pain, not their lives. But they have given up hope that they or anyone else can help them.
Myth: People often die by suicide “on a whim.”
FACT: There is almost always evidence of prior planning. Mental preparation for the actual suicide event is an essential characteristic of the phenomenon. In some cases, planning may be “shelved” for a period of time
|
Glossary of Terms when dealing with Self-Directed Violence
THOUGHTS
1. Non-Suicidal Self-Directed Violence Ideation
Self-reported thoughts regarding a person’s desire to engage in self-inflicted potentially injurious behavior. There is no evidence of suicidal intent. For example, persons engage in Non-Suicidal Self-Directed Violence Ideation in order to attain some other end (e.g., to seek help, regulate negative mood, punish others, to receive attention).
2. Suicidal Ideation
Thoughts of engaging in suicide-related behavior. For example, intrusive thoughts of suicide without the wish to die would be classified as Suicidal Ideation, Without Intent.
3. Non-Suicidal Self-Directed Violence, Preparatory
Acts or preparation towards engaging in Self-Directed Violence, but before potential for injury has begun. This can include anything beyond a verbalization or thought, such as assembling a method (e.g., buying a gun, collecting pills) or preparing for one’s death by suicide (e.g., writing a suicide note, giving things away). For example, hoarding medication for the purpose of overdosing would be classified as Suicidal Self-Directed Violence, Preparatory.
4. Non-Suicidal Self-Directed Violence
Behavior that is self-directed and deliberately results in injury or the potential for injury to oneself. There is no evidence, whether implicit or explicit, of suicidal intent. For example, persons engage in Non-Suicidal Self-Directed Violence in order to attain some other end (e.g., to seek help, regulate negative mood, punish others, to receive attention).
BEHAVIORS
5. Undetermined Self-Directed Violence
Behavior that is self-directed and deliberately results in injury or the potential for injury to oneself. Suicidal intent is unclear based upon the available evidence. For example, the person is unable to admit positively to the intent to die (e.g., unconsciousness, incapacitation, intoxication, acute psychosis, disorientation, or death); OR the person is reluctant to admit positively to the intent to die for other or unknown reasons.
6. Suicidal Self-Directed Violence
Behavior that is self-directed and deliberately results in injury or the potential for injury to oneself. There is evidence, whether implicit or explicit, of suicidal intent. For example, a person with the wish to die cutting her wrists with a knife would be classified as Suicide Attempt, With Injury.
Key Terms when Dealing with Self-Directed Violence
Self-Directed Violence: Behavior that is self-directed and deliberately results in injury or the potential for injury to oneself.
Suicidal Intent: There is past or present evidence (implicit or explicit) that an individual has a wish to die, means to kill him/herself, and understands the probable consequences of his/her actions or potential actions. Suicidal intent can be determined retrospectively and in the absence of suicidal behavior.
Physical Injury: A (suspected) bodily lesion resulting from acute overexposure to energy (this can be mechanical, thermal, electrical, chemical, or radiant) interacting with the body in amounts or rates that exceed the threshold of physiological tolerance. In some cases, an injury results from an insufficiency of vital elements, such as oxygen. Acute poisonings and toxic effects, including overdoses of substances and wrong substances given or taken in error are included, as are adverse effects and complications of therapeutic, surgical and medical care. Psychological injury is excluded in this context.
Interrupted by Self or Other: A person takes steps to injure self but is stopped by self/another person prior to fatal injury. The interruption may occur at any point.
Suicide Attempt: A non-fatal self-inflicted potentially injurious behavior with any intent to die as a result of the behavior.
Suicide: Death caused by self-inflicted injurious behavior with any intent to die as a result of the behavior.
|
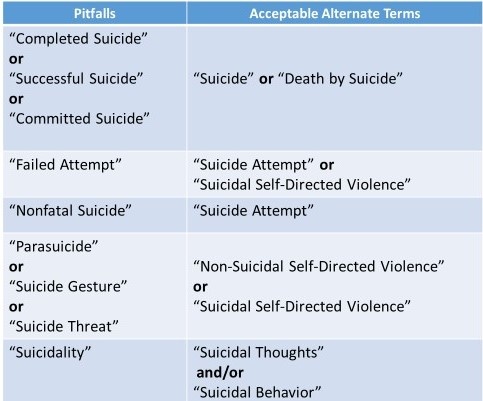
Appropriate Nomenclature for Suicide
|
Defining the Problem
- Attempted suicide is a potentially self-injurious act committed with at least some intent to die as a result of the act.
- Suicide is an attempt to solve a problem of intense emotional pain with impaired problem-solving skills.
- Individuals of all races, creeds, incomes, and educational levels die by suicide. There is no typical suicide victim.
Characteristics of Suicide
Alternative to problem perceived as unsolvable by any other means:
Viewing suicide from this perspective has several important implications.
1.For one, just as someone may get a temporary high from a drug, he or she may obtain temporary attention, support, or even popularity after a suicide attempt.
2.A second implication of viewing suicide as an alternative is that suicide can then be understood as less than a wish to die than a wish to escape the intense emotional pain generate from what appears to be an inescapable solution.
Person is often ambivalent:
What this means is that the people are feeling two things at the same time: there is a part of them that wants to die and part that wants to live and both parts must be acknowledged.
While they line up with and unequivocally supports the side that wants to live, this can’t be done by ignoring or dismissing that side that wants to die.
Suicidal solution has an irrational component:
People who are suicidal are often unaware of the consequences of suicide that are obvious to the rest of the word. For example, they are usually not thinking about the impact of their death on others, or they hold a perception they will be reincarnated or somehow still present to see how others react to their deaths.This irrationality affects how trapped and helpless the person feels.
Suicide is a form of communication:
For people who are suicidal, normal communication has usually broken down and the suicide attempt may be their way of sending a message or reacting to the isolation they feel because their communication skills are ineffective.
|
Risk Factors for Suicide
Risk factors may be thought of as leading to or being associated with suicide; that is, people “possessing” the risk factors are at greater potential for suicidal behavior.
- Bio-psychosocial
- Environmental
- Socio-cultural
Bio-psychosocial Risk Factors
- Mental disorders, particularly mood disorders, schizophrenia, anxiety disorders and certain personality disorders
- Alcohol and other substance use disorders
- Hopelessness
- Impulsive and/or aggressive tendencies
- History of trauma or abuse
- Some major physical illnesses
- Previous suicide attempt
- Family history of suicide
Environmental Risk Factors
- Job, financial loss, drop out of school
- Homelessness
- Relational or social loss
- Easy access to lethal means
- Local clusters of suicides that have a contagious influence
Socio-cultural Risk Factors
- Lack of Social Support : Isolation can lead to feelings of alienation and depression that may ultimately lead to suicidal thoughts and behaviors, research has shown that social support can help prevent someone moving from suicidal ideation to suicide attempts.
- Membership in Repressive Group: group membership can come with a price. Groups sometimes require stress-inducing obligations and high levels of commitment; and they may lead people to adopt behavioral and attitudinal norms (rather than thinking for themselves). These types of groups can feel repressive and stifling and may actually contribute to suicidal thoughts and feelings. In extreme cases, groups can even demand that someone sacrifice him or herself for the "greater good.“
- Social Norms: Social norms regarding suicide can influence its meaning (i.e., whether it is stigmatized) as well as its frequency. Many societies and religious traditions ban suicide and view it as a sin or taboo behavior. Others portray suicide as a legitimate behavior in certain circumstances. For instance, some Islamic groups promote suicide as a means of martyrdom in a war against an enemy. Among Buddhist monks, self-sacrifice for religious reasons can be viewed as an honorable act. In India, it is acceptable for a widow to burn herself on her husband's funeral pyre. The Hindu code of conduct condones suicide for incurable diseases or as a response to great misfortune.
Youth Specific Youth Factors
- Divorce or separation of parents
- Harassment by peers (bullying)
- Sexual identity crisis
- Gay, lesbian, bisexual or transgender sexual orientation
- Easy access to lethal methods, especially guns
- School crisis (disciplinary, academic)
- Genetic predisposition (serotonin depletion)
- Feelings of isolation or being cut off from others
- Ineffective coping mechanisms
- Inadequate problem-solving skills
- Cultural and/or religious beliefs (e.g., belief that suicide is a noble or acceptable solution to a personal dilemma)
- Exposure to suicide and/or family history of suicide
- Influence (either through personal contact or media representations) of significant people who died by suicide
- Loss or separation (e.g., death, divorce, relationships)
- Exposure to violence
- Family crisis (e.g., abuse, domestic violence, running away, child-parental conflict
- Barriers to receiving mental health treatment; stigma, affordability, availability, accessibility
- Experiences of disappointment or rejection
- Feelings of stress brought about by perceived achievement needs
- Unwanted pregnancy, abortion
- Infection with HIV or other STDs
- Serious injury that may change life course (i.e., traumatic brain injury)
- Severe or physical terminal illness, or mental illness or substance abuse
|
Suicidal Warning Signs
- Threatening to hurt or kill oneself or talking about wanting to hurt or kill oneself
- Looking for ways to kill oneself by seeking access to firearms, pills, or other means
- Talking or writing about death, dying, or suicide when these actions are out of the ordinary for the person
- Feeling hopeless
- Feeling rage or uncontrolled anger or seeking revenge
- Acting reckless or engaging in risk activities – seemingly without thinking
Warning Signs for Youth Suicide
- Suicide threats
- uicide plan/method/access
- Making final arrangements
- Sudden changes in physical habits and appearance
- Preoccupation with death and suicide themes
- Increased inability to concentrate or think clearly
- Loss of interest in previously pleasurable activities
- Symptoms of depression
- Increase use and abuse of alcohol and/or drugs
- Hopelessness
- Rage, anger, seeking revenge
- Reckless behavior or activities
- Feeling trapped
- Anxiety and agitation
- Sleep difficulties, especially insomnia
- Dramatic changes in mood
- Sudden/recent purchase of a weapon
- No reason for living
- No sense of purpose in life
- Sense of being a burden
- Profound sense of loneliness, alienation and isolation
- Sense of fearlessness
|
Worldwide Facts About Suicide
- In our world, every year, over 800,000 people die from suicide; this roughly corresponds to one death every 40 seconds.
- The number of lives lost each year through suicide exceeds the number of deaths due to homicide and war combined.
- In 2012, suicide accounted for 1.4% of all deaths worldwide, making it the 15th leading cause of death.
- Suicide is the fifth leading causes of death among those aged 30-49 years in 2012 globally.
- Overall, it is estimated that during 2012 for each adult who died of suicide there were over 20 others who made suicide attempts.
- The psychological pain that leads each of these individuals to take their lives is unimaginable.
- Mental disorders (particularly depression and alcohol use disorders) are a major risk factor for suicide in Europe and North America; however, in Asian countries impulsiveness plays an important role.
- •Suicide is complex with psychological, social, biological, cultural and environmental factors involved.
- Connectedness is crucial to individuals who may be vulnerable to suicide.
- Studies have shown that social isolation can increase the risk of suicide and, conversely, that having strong human bonds can be protective against it.
- Reaching out to those who have become disconnected from others and offering them support and friendship may be a life-saving act.
- Connectedness can also be understood in terms of clinical care. Mental illness, particularly depression, is an important risk factor for suicide.
|
United States Suicide Statistics
- 1 suicide every 12.8 minutes
- 13 per 100,000
- 24% rise from 1999-2014
- Approximately 8-25 attempted suicides for every suicide death
- Adults have the highest number of suicides.
- Second leading cause of death among ages 25 – 34.
- In 2007, approximately 69% of all suicides in Florida were among ages 25 – 64.
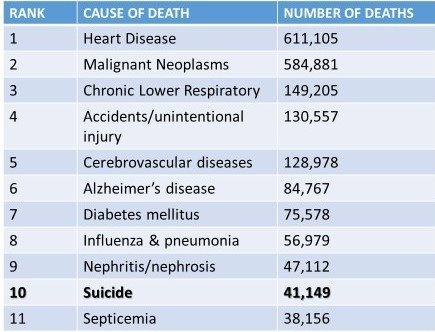
Of the leading causes of death in United States (2013) Suicide ranked 10th of all causes
|
Youth Suicide Statistics
- Third leading cause of death for ages 10 – 24 (only accidents and homicide occur more in this age).
- Second leading cause of death for American college students.
- More teenagers and young adults die from suicide than from cancer, heart disease, AIDS, birth defects, stroke, pneumonia, influenza, and chronic lung disease combined.
- Everyday across the nation, there are approximately 12 youth suicides.
- Every 2 hours, 11 minutes, a person under the age of 25 dies by suicide in the United States.
- In the U.S. in 2005, 32,637 people died by suicide. Of these, 4,212 deaths were by people between the ages of 15 – 24.
- For every suicide by youth, it is estimated that 100-200 attempts are made.
- Firearms are the most commonly used suicide method accounting for 49% of suicide deaths.
- For the past 60 years, the suicide rate has quadrupled for makes 15 – 24 years old and doubled for females of the same age.
|
Death by Suicide and Psychiatric Diagnosis
Psychological autopsy studies done in various countries from over almost 50 years report the same outcomes.
- 90% of people who die by suicide are suffering from one or more psychiatric disorders:
- Major Depressive Disorder
- Bipolar Disorder, Depressive Phase
- Alcohol or Substance Abuse
- Schizophrenia
- Personality Disorders such as Borderline Personality Disorder
Signs of Depression
When diagnosing depression, usually there must be a marked behavioral change lasting for two weeks or longer which can include all or some of the following signs:
-Loss of interest in normal daily activities
-Feeling sad or down
-Feeling hopeless
-Crying spells for no apparent reason
-Problems sleeping
-Trouble focusing or concentrating
-Difficulty making decisions
-Unintentional weight gain or loss
-Irritability
-Restlessness
-Being easily annoyed
-Feeling fatigued or weak
-Feeling worthless
-Loss of interest in sex
-Thoughts of suicide or suicidal behavior
-Unexplained physical problems, such as back pain or headaches
Signs of Depression in Youth:
Oversensitivity to criticism
Risk-taking, hyperactivity
Low self-esteem
Indecision, withdrawal, inactivity
Somatic symptoms and complaints
Aggression, hostility
Sleep disturbances
Eating disorders
Four out of ten children and adolescents will have a second episode of depression within two years.
Depressed adolescents are at an increased risk for substance abuse and pregnancy.
Over half of depressed youth will attempt suicide, and at least 7% will ultimately die as a result.
Early identification and treatment of depression can save lives.
|
How to go about assessing suicide ideation
Clients should be directly asked if they have thoughts of suicide and to describe them. The evaluation of suicidal thoughts should include the following:
- Onset (When did it begin)
- Duration (Acute, Chronic, Recurrent) Intensity (Fleeting, Nagging, Intense)
- Frequency (Rare, Intermittent, Daily, Unabating)
- Active or passive nature of the ideation (‘Wish I was dead’ vs. ‘Thinking of killing myself’)
- Whether the individual wishes to kill him/her self, or is thinking about or engaging in potentially dangerous behavior for some other reason (e.g., cutting oneself as a means of relieving emotional distress)
- Lethality of the plan (No plan, Overdose, Hanging, Firearm)
- Triggering events or stressors (Relationship, Illness, Loss)
- What intensifies the thoughts
- What distract the thoughts
- Association with states of intoxication (Are episodes of ideation present or exacerbated only when individual is intoxicated? This does not make them less serious; however, may provide a specific target for treatment)
- Understanding regarding the consequences of future potential actions
Example of Questions on Ideation:“With everything that has been going on, have you been experiencing any thoughts of killing yourself?”
- When did you begin having suicidal thoughts?
- Did any event (stressor) precipitate the thoughts?
- How often do you have thoughts of suicide?
- How long do they last?
- How strong are the thoughts of suicide?
- What is the worst they have ever been?
- What do you do when you have these (suicidal) thoughts?
- What did you do when they were the strongest ever?
- Do thoughts occur or intensify when you drink or use drugs?
When considering suicidal intent - assess for past or present evidence (implicit or explicit) that the individual wishes to die, means to kill him/herself, and understands the probable consequences of his/her actions or potential actions.
Assessing for current intent and the degree of intent for suicide is a key component of the assessment process. The presence of intent to act upon suicidal thoughts is generally indicative of high risk for suicide. Therefore, it is important to understand the extent to which the client: 1) wishes to die; 2) means to kill him/herself; 3) and understands the probable consequences of his/her actions or potential actions.
Clients with active suicidal ideation may have the intent to act, a plan to act, both, or neither. The evolution of intent can occur over minutes or years. In some cases, the intent stage may be very brief and the suicidal ideation may propel to a behavior or suicide act.
1. Clients should be asked the degree to which they wish to die, mean to kill him/herself, and understand the probable consequences of his/her actions or potential actions
2. The evaluation of intent to die should be characterized by:
- Strength of the desire to die
- Strength of determination to act
- Strength of impulse to act or ability to resist the impulse to act
3. The evaluation of suicidal intent should be based on indication that the individual:
- Wishes to die
- Means to kill him/herself
- Understands the probable consequences of the actions or potential actions
- These factors may be highlighted by querying regarding how much the individual has thought about a lethal plan, has the ability to engage that plan, and is likely to carry out the plan
Example of Questions on Intent:
- Do you wish you were dead?
- Do you intend to try to kill yourself?
- Do you have a plan regarding how you might kill yourself?
- Have you taken any actions towards putting that plan in place?
- How likely do you think it is that you will carry out your plans?
Assess if the patient has begun to show actual behavior of preparation for engaging in Self-Directed Violence (e.g., assembling a method, preparing for one’s death).
Assessment of risk for suicide may find that the client has already begun to take specific action in implementing a plan to kill him/herself (e.g., buying a gun, collecting pills, assembling methods), or started to make preparation for the aftermath of their death (e.g., giving away belongings, changing a will, or sending notes to loved ones). These acts and behaviors are defined as preparatory behaviors and put the cltient at the high risk for suicide. Research has shown that resolved plans and preparatory behavior predicted death by suicide and history of suicide attempts.
Gathering information regarding preparatory behaviors may require exploring other sources of information about the cltient. This may require a careful discussion with the client and obtaining the client’s consent. Peers, family members, work and social or community associations may play a critical role in corroborating information regarding psychosocial functioning and preparatory behavior.
Clinicians should evaluate preparatory behaviors by inquiring about:
A. Preparatory behavior like practicing a suicide plan. For example:
- Mentally walking through the attempt
- Walking to the bridge
- Handling the weapon
- Researching for methods on the internet
B. Thoughts about where they would do it and the likelihood of being found or interrupted?
C. Action to seek access to lethal means or explore the lethality of means. For example:
- Acquiring a firearm or ammunition
- Hoarding medication
- Purchasing a rope, blade, etc.
- Researching ways to kill oneself on the internet
C. Action taken or other steps in preparing to end one’s life:
- Writing a will, suicide note
- Giving away possessing
- Reviewing life insurance policy
D. Obtain collateral information from sources such as family members, medical records, and therapists.
Examples of Questions on Preparation:
- Do you have a plan or have you been planning to kill yourself? If so, how would you do it? Where would you do it?
- Do you have the (drugs, gun, rope) that you would use? Where is it right now?
- Do you have a timeline in mind for killing yourself?
- Is there something (an event) that would trigger acting on the plan?
- How confident are you that your plan will end your life?
- What have you done to begin to carry out the plan?
- Have you made other preparations (e.g., updated life insurance, made arrangements for pets)?
Previous Suicide Attempt
Obtain information from the client and other sources about previous suicide attempts. Historical suicide attempts may or may not have resulted in injury, and may have been interrupted by the client or by another person prior to fatal injury.
In making assessment of the risk for suicide if there was a previous suicide attempt
The assessment of risk for suicide should include information from the patient and collateral sources about previous suicide attempt and circumstances surrounding the event (i.e., triggering events, method used, consequences of behavior, role of substances of abuse) to determine the lethality of any previous attempt:
- Inquire if the attempt was interrupted by self or other, and other evidence of effort to isolate or prevent discovery
- Inquire about other previous and possible multiple attempts
- For patients who have evidence of previous interrupted (by self or other) attempts, obtain additional details to determine factors that enabled the patient to resist the impulse to act (if self-interrupted) and prevent future attempts.
Warning Signs – Indications for Urgent/Immediate Action
There is a need to recognize precipitating emotions, thoughts, or behaviors that are most proximally associated with a suicidal act and reflect high risk
Many suicidal individuals reveal warning signs or signals of their intention to engage suicidal behaviors, thereby providing clinicians or other supportive persons the opportunity to recognize an impending suicidal crisis and intervene.
Three direct warning signs portend the highest likelihood of suicidal behaviors occurring in the near future. Observing these warning signs warrants immediate attention, mental health evaluation, referral, or consideration of hospitalization to ensure the safety, stability and security of the individual:
First Warning Sign: Suicidal communication – writing or talking about suicide, wish to die, or death (threatening to hurt or kill self).
Second Warning Sign: Seeking access or recent use of lethal means: such as weapons, medications, or other lethal means
Third Warning Sign: Preparations for suicide – evidence or expression of suicide intent, and/or taking steps towards implementation of a plan. Makes arrangements to divest responsibility for dependent others (children, pets, elders), or making other preparations such as updating wills, making financial arrangements for paying bills, saying goodbye to loved ones, etc.
These signals are likely to be even more dangerous if the person has previously attempted suicide, has a family history of suicide and/or intends to use a method that is lethal and to which he/she has access. Other indirect warning sign presentation(s) or behavioral expressions that may indicate increased suicide risk and urgency in a patient at risk for suicide
Assessing These Warning Signs
In order to assess for other warning signs that may indicate likelihood of suicidal behaviors occurring in the near future, and require immediate attention it is important to assess the client for any or all of the following negative contributing factors:
- Substance abuse – increasing or excessive substance use (alcohol, drugs, smoking)
- Hopelessness – expresses feeling that nothing can be done to improve the situation
- Purposelessness – express no sense of purpose, no reason for living, decreased self-esteem
- Anger – rage, seeking revenge
- Recklessness – engaging impulsively in risky behavior
- Feeling Trapped – expressing feelings of being trapped with no way out
- Social Withdrawal – withdrawing from family, friends, society
- Anxiety – agitation, irritability, angry outbursts, feeling like wants to “jump out of my skin”
- Mood changes – dramatic changes in mood, lack of interest in usual activities/friends
- Sleep Disturbances – insomnia, unable to sleep or sleeping all the time
- Guilt or Shame – Expressing overwhelming self-blame or remorse
- Sense of being a burden – feeling that their lives are a burden for others to put up with
Assessment of Factors that Contribute to the Risk for Suicide
Assess factors that are known to be associated with suicide (i.e., risk factors, precipitants) and those that may decrease the risk (i.e., protective factors).
Steps needing to be taken in assessment:
1. Obtain information about risk factors during a baseline evaluation – recognizing that risk factors have limited utility in predicting future behavior.
2. Draw on available information including prior history available in the client’s record, inquiry and observation of the patient, family or military unit members and other sources where available.
3. Assessment tools may be used to evaluate risk factors, in addition to the clinical interview, although there is insufficient evidence to recommend one tool over another.
4. The baseline assessment should include information about risk factors sufficient to inform further assessment if conditions change such as firearm in the home, social isolation, history of depression, etc.
5. Risk factors should be considered to denote higher risk individuals (e.g., those with a history of depression) and higher risk periods (e.g., recent interpersonal difficulties).
6. Risk factors should be solicited and considered in the formulation of a client’s care.
7. Reassessment of risk should occur when there is a change in the client’s condition (e.g., relapse of alcoholism) or psychosocial situation (e.g., break-up of intimate relationship) to suggest increased risk. Information needs to updated about risk factors when there are changes in the individual’s symptoms or circumstances to suggest increased risk.
8. Patients ages 18 to 25 who are prescribed an antidepressant are at increased risk for suicidal ideation and warrant increase in the frequency of monitoring for such behavior
9. For a Military Service person in transition there is a need to:
- Inquire about changes in the client’s life and be aware of other indicators of change (retirement physical, overseas duty screening, etc.).
- Be willing to discuss and consider methods to strengthen social support during the transition time if there are other risk factors present.
|
Risk Factors
Risk factors distinguish a higher risk group from a lower risk group. Risk factors may be modifiable or non-modifiable and both inform the formulation of risk for suicide. Modifiable risk factors may also be targets of intervention.
Psychological Factors
- Suicide of relative, someone famous, or a peer
- Suicide bereavement
- Loss of loved one (grief)
- Loss of relationship (divorce, separation)
- Loss of status/respect/rank (public humiliation, being bullied or abused, failure work/task)
Social Factors
Stressful Life Events (acute experiences)
- Breakups and other threats to prized relationships
- Other events (e.g., fired, arrested, evicted, assaulted)
- Chronic Stressors (ongoing difficulties)
Financial Problems
- Unemployment, underemployment
- Unstable housing, homeless
- Excessive debt, poor finances (foreclosure, alimony, child support)
Legal Problems (difficulties)
- DUI/DWI
- Lawsuit
- Criminal offence and incarceration
Social Support
- Poor interpersonal relationship (partner, parents, children)
- Geographic isolation from support
Barriers to accessing mental health care
Recent change in level of care (discharge from inpatient psychiatry)
Mental Disorders
Mood or affective disorder (major depression, bipolar, post-partum)
Personality disorder (especially borderline and antisocial)
Schizophrenia
Anxiety (PTSD, Panic)
Substance Use Disorder (alcohol, illicit drugs, nicotine)
Eating disorder
Sleep disturbance or disorder
Trauma (psychological)
Medical Conditions
History of Traumatic Brain Injury (TBI)
Terminal disease
HIV/AIDS
New diagnosis of major illness
Having a medical condition
Worsening of chronic illness
Intoxication
Substance withdrawal (alcohol, opiates, cocaine, amphetamines)
Use of prescribed medication w/ warning for increased risk of suicide
Physical Symptoms
- Chronic pain
- Insomnia
- Function limitation
Military Specific
Disciplinary actions (UCMJ, NJP)
Reduction in rank
Career threatening change in fitness for duty
Perceived sense of injustice or betrayal (unit/command)
Command/leadership stress, isolation from unit
Transferring duty station (PCS)
Administrative separation from service/unit
Adverse deployment experience
Deployment to a combat theater
Pre-existing & Non-modifiable
Age (young & elderly)
Gender (male)
Race (white)
Marital status (divorce, separate, widowed)
Lower education level
Same sex orientation (LGBT)
Cultural or religious beliefs
Family history of:
- Suicide/ attempt
- Mental illness (including SUD)
- Child maltreatment trauma-physical/psychological/sexual
- Sexual trauma
Protective Factors
Protective factors are capacities, qualities, environmental and personal resources that drive individuals towards growth, stability, and health and may reduce the risk for suicide.
Assessment should include evaluation of protective factors, patient’s reason to for living, or other factors that mitigate the risk for suicide.
Social Context Support System
Strong interpersonal bonds to family/unit members and community support
Employed
Intact marriage
Child rearing responsibilities
Responsibilities/duties to others
A reasonably safe and stable environment
Positive Personal Traits
Help seeking
Good impulse control
Good skills in problem solving, coping and conflict resolution
Sense of belonging, sense of identity, and good self-esteem
Cultural, spiritual, and religious beliefs about the meaning and value of life
Optimistic outlook – Identification of future goals
Constructive use of leisure time (enjoyable activities)
Resilience
Access to Health Care
Support through ongoing medical and mental health care relationships
Effective clinical care for mental, physical and substance use disorders
Good treatment engagement and a sense of the importance of health and wellness
Note: This section on Assessment of Risk, was adapted from the VA/DoD (2013). Clinical Practice Guideline for Assessment and Management of Patients at Risk for Suicide. Washington, DC: The Office of Quality Safety and Value and Quality Management Division, United States Army MEDCOM. Available at: http://www.healthquality.va.gov/guidelines/MH/srb/VADODCP_SuicideRisk_Full.pdf on the VA/DoD Clinical Practice Guidelines section at: http://www.healthquality.va.gov/guidelines/MH/srb/
|
How do you Remember the Warning Signs of Suicide?
Here’s an Easy-to-Remember Mnemonic:
|
IS PATH WARM?
I Ideation
S Substance Abuse
P Purposelessness
A Anxiety
T Trapped
H Hopelessness
W Withdrawal
A Anger
R Recklessness
M Mood Change
|
A person in acute risk for suicidal behavior most often will show:
Warning Signs of Acute Risk:
- Threatening to hurt or kill him or herself, or talking of wanting to hurt or kill him/herself; and/or,
- Looking for ways to kill him/herself by seeking access to firearms, available pills, or other means; and/or,
- Talking or writing about death, dying or suicide, when these actions are out of the ordinary.
These might be remembered as expressed or communicated IDEATION. If observed, seek help as soon as possible by contacting a mental health professional.
Additional Warning Signs:
- Increased SUBSTANCE (alcohol or drug) use
- No reason for living; no sense of PURPOSE in life
- ANXIETY, agitation, unable to sleep or sleeping all the time
- Feeling TRAPPED - like there’s no way out
- HOPELESSNESS
- WITHDRAWING from friends, family and society
- Rage, uncontrolled ANGER, seeking revenge
- Acting RECKLESS or engaging in risky activities, seemingly without thinking
- Dramatic MOOD changes
If observed, seek help as soon as possible by contacting a mental health professional
Note:This section was adapted from the American Association of Suicidology website at: http://www.suicidology.org/resources/warning-signs
|
|
|