Psychopharmacology 101
For Non-prescribing
Mental Health Professionals -
A Training Resource
By Jim Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
Resource for Mental Health Professionals:
|
Anxiety Disorders
Current Medications for Anxiety Disorders
|
Classification
|
Generic Name (Brand Name)
|
|
New Benzodiazepines
|
Lorazepam (Ativan)
Alprazolam (Xanax)
|
|
Old Benzodiazepines
|
Diazepam (Valium)
Chlordiazeproxide (Librium)
Clonazepam (Klonopin)
Temazepam) (Restoril)
Triazolam (Halcion)
|
|
Buspirone
|
Buspirone (Buspar)
|
|
SSRI’s
|
Escitalopram (Lexapro)
Paroxetine (Paxil)
|
|
SNRI
|
Venlafaxine (Effexor XR)
|
|
Beta Blockers
|
Propranolol (Inderal)
Metoprolol (Lopressor)
Atenolol (Tenormin)
|
|
Sleep Medications (z Drugs)
|
Zolpidem (Ambien)
Zaleplon (Sonata)
Eszopiclone (Lunesta)
|
Specific Medications Treatments by Anxiety Disorders
- GAD: Paroxetine, Escitalopram, Venlafaxine, Duloxetine, Alprazolam
- Panic Disorder: Fluoxetine, Paroxetine, Sertraline, Venlafaxine, Alprazolam, Clonazepam
- Social Anxiety Disorder: Paroxetine, Sertraline, Venlafaxine, Fluvoxamine
- PTSD: Paroxetine, Sertraline
- OCD: Sertraline, Paroxetine, Fluoxetine, Fluvoxamine, Clomipramine
- The Phobias: Phenelzine/Nardil®,Exposure therapy,MOA: MAOI – food limitations
Background
Many of clients are using medications and they frequently come to therapists already on medications. Why? As many as 95% of clients with panic disorder first seek treatment from their primary care physician. Clients with anxiety disorders are less likely to go to psychiatrist and most likely to get meds from primary care doctor. Therapists may have little direct influence over whether meds are first prescribed, but should provide education about meds. What do therapists need to tell their clients, and how can they make sure that their explanations are factually correct and promote responsiveness to and engagement in treatment?
It would be a mistake not to consider how being prescribed medication affects treatment and it is Important for therapists to understand the effects, side effects, and method of action of meds. Therapists must recognize that being prescribed meds often suggests to clients that therapy is not necessary. Client’s preferences and expectations about medication should be considered because their motivation and engagement can be impacted. Therapists' attitudes toward medication influence clients' response to medication as well.. Therapist’s role in providing credible rationale is essential in obtaining the beneficial effects of medication.
What is Anxiety?
Is anxiety the “most medical” of the psychological problems?
Neurobiology: Hyperarousal
Brainstem reticular formation:
- Locus coeruleus: Norepinephrine; Dorsal/Medial Raphe Nuclei: Serotonin
Pathophysiology
- Noradrenergic model
- GABA receptor model
- Serotonin 5-HT model
- Dysregulation of hypothalamicpituitary-adrenal axis
Therapist can be a resource because they can:
- Recommend when clients should seek medication or changes in medication, based on professional observation
- Provide information about the expected effects of medications- long term perspective is helpful
- Provide information about side effects and contraindications
- Clarify that there are no skills developed as a result of medication use
- Provide information on effect of medication on therapeutic interventions
- Provide feedback on the effectiveness or impact of a medication on specific clients' behaviors
- Help clients identify and communicate symptoms, concerns, questions to the prescriber.
-
Help clients recognize that the goal of treatment is NOT to eliminate anxiety but to recognize that anxiety is a normal, protective, innate response that is often useful.
-
Acknowledge that clients’ physical symptoms need to be acknowledged as real, but recognized as not always indicating the clients are in danger.
-
Avoid catastrophic interpretations of anxiety as “going crazy” or “a heart attack” and need to empathically challenge that anxiety is not dangerous.
-
Reasure clients that management of anxiety is the goal and is not relieving anxiety and that the occurrence of anxiety does not indicate failure of treatment.
-
Point out that medication can have negative effects as well as positive ones and that medication can have negative as well as positive effects on therapy.
-
Explain to clients that exposure treatment is one of the most potent treatments available, but that it must generate feelings of anxiety for it to be effective.
- Explan that there is no evidence that a chemical imbalance causes anxiety which is something that many clients are told.
-
Nevertheless, they can reasure clients that the right medications do help clients cope with anxiety, and may promote desired changes in behavior that help rewire the brain. But that medications can also interfere with learning and rewiring
For Clients who are “against” medication use Therapists can help clients:
- Explore their perspectives on medication
- Correct misperceptions that they have about medication
- Explaining that they do not need to see themselves as weak or damaged if medication is part of their treatment
- Presenting medication as a “tool” in recovery which is important
- Explaining *how* medications affect the brain and will help rewire their future responses to anxiety
- Reassuring them that medicine is not able to change the brain itself in durable, helpful ways without their involvement and assistance
- Understand that they need to work with the medication, and use it in informed ways
Benzodiazepines (BZD)
- Lorezepam (Ativan)
- Alprazolam (Xanax)
- Diazepam (Valium)
- Chlordiazeproxide (Librium)
- Clonazepam (Klonopin)
- Temazepam (Restoril)
Caution in Use of Benzodiazepines BZD's
- Psychoactive: Acute effects, rapid change in mood or thought; Highly addictive, not for long term use; Risk for fatality in overdose when combined with alcohol (respiratory depression)
- Schedule IV Drug
- Paradoxical reaction: disinhibition: impulse control issues
- Do not use more than 2-4 Weeks; No utility for anxiety after 4 months & Sleep disorders after 3-14 days
- Long term effects: Depression; Emotional blunting; Suicidal behavior; Memory problems; Psychomotor Retardation & Dis-inhibition, possible aggression
- Tolerance and dependence can occur - Dependency associated with dose and duration
- Time-limited use
- DANGER! If combined with alcohol
- Avoid abrupt cessation to reduce seizure risk
|
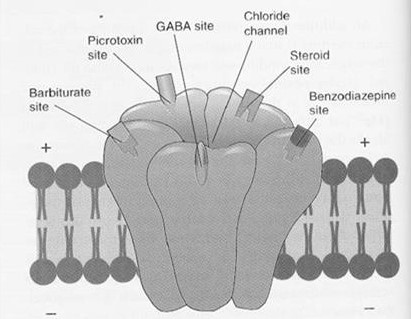
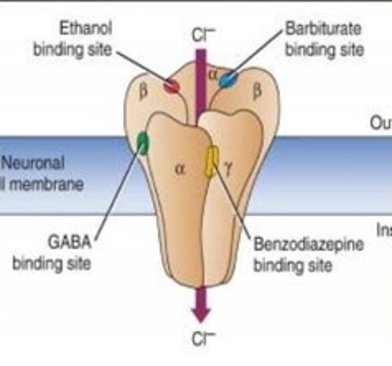
Benzodiazepines Mechanism of Action
Allosteric modulators of the GABA-a chloride ionophore
NOTE: BZD agonist, not completely accurate
|
How Do Benzodiazepines BZD's Work?
Considered minor tranquilizers, because like GABA (gamma amino butyric acid) they bind to GABA receptor sites and add to the inhibitory effect of GABA, which is accomplished by opening chloride channels (Cl-) in a neuron. They basically inhibit neurons, making them less likely to fire. They are a central nervous system depressant creating effects that vary from mild impairment to hypnosis. They produce widespread effects in the brain, as well as the body, creating sedation, impairing memory, influencing perceptions. They reduce anxiety by inhibiting the neural processes that create it.
|
How to Explain Benzodiazepines Effects to Clients
- Clients readily recognize the sedating effect
- Concern should be raised about effect on rewiring brain - decreasing activation has consequences…
- They interfere with the brain learning because the neurons can’t change when they are inhibited-- Students don’t learn when they are asleep
- Remember “activate to generate” new connections
- So while they sedate the brain and reduce anxiety, they interfere with making changes in the brain-- this is why they should only be a temporary solution
- As noted, they also have addictive properties, and withdrawal symptoms can be worse than the original anxiety, something clients should be told
-
Recommendations are that Benzodiazepines only be administered during acute phases of anxiety disorders, but their use is still increasing
-
Please help minimize their use!
-
The Physician Drug Referemce clearly states their use should be time-limited (4 to 6 weeks) but addiction can occur before 6 weeks!
- Signs of physical dependence occur as soon as 2 weeks- tapering becomes necessary
- Most appropriately prescribed for use *when needed* and not as a daily medication
-
Important: Use of these meds along with opioids has high risks and can result in fatalities
How to explain Effect of Benzodiazepines on Anxiety Reduction Therapy
- BDZ's are designed to inhibit or put to sleep certain parts of one's nervous system in a rather quick way – producing relief
- The amygdala is kept from responding, because it is basically asleep and can’t create anxiety and all the associated physical responses
- Unfortunately because the amygdala – and other parts of the brain- are asleep, it doesn’t allow the brain to learn anything– so it can keep therapy, especially exposure therapy, from being effective
- It can’t be targeted and has widespread effects in one's body
- It is also addictive, and can end up producing more anxiety (rebound anxiety) when one tries to stop taking it
When do Benzodiazepines fit in?
- Psychiatrists are more likely to prescribe them than primary care physicians, and when they feel regular dosing is required, they prescribe clonazepam rather than alprazolam or others
- Clonazepan (Klonopin) is no less addictive, however
- Often used along with SSRIs, SNRIs when first prescribed, to reduce side effect of anxiety that occurs initially
- They interfere with the effectiveness of exposure therapy methods so should be discontinued to achieve best results
- But, still Benzodiazepine benefits are rarely offset by the side effects, risks, and rebound symptoms
Benefits of Benzodiazepines:
- Very rapid relief from anxiety – can use on as-needed basis
- Preferred by clients over SSRIs
- Combined with SSRIs/SNRIs to reduce initial anxiety side effects
Disadvantages/Risks:
- Side effects of sedation, dizziness, depression, nausea, muscle weakness, memory problems, coordination problems
- Combining with alcohol or opioids can be fatal
- Risk of physiological dependence and addiction
- Recommendation to limit to short term use only – dependence can develop in 4-6 weeks with daily use
- Long term use can result in impairment in cognitive skills, such as verbal learning, memory
- Severe withdrawal symptoms likely in at least 30% of individuals with muscle spasms, gastrointestinal problems, rebound anxiety, depression
|
Benzodiazepines Withdrawal
- Anxiety/Depression
- Perceptual Disturbances
- Sleep Disturbance
- Tremor/Shakiness/Twitches
- Muscle aches and pains
- Hypersensitivity to touch
- Risk of suicide and self-harming behaviors (especially in young people)
Why Benzodiazepine Use Should be Minimized
- As the drugs that most quickly reduce anxiety, these drugs are often preferred by clients
- But other interventions are effective including relaxation, exercise, meditation, and they do not have detrimental side effects
- Benzodiazepines have a variety of negative effects
- A tendency for dependence to develop quickly (within 4 weeks)
- Well documented adverse cognitive effects on memory and learning
- Interference with effectiveness of treatments such as exposure
- An increased risk of falls and impaired driving in older adults
- Risks of cognitive dysfunction, behavioral problems when taken with alcohol
- Discontinuation difficulties that include insomnia, gastrointestinal symptoms, agitation, rebound anxiety
- The goal should always be to eliminate benzodiazepine use or restrict it to intermittent use that prevents dependency
|
Buspirone
Brand Names: Buspar, Buspar Dividose, Vanspar
What type of drug is Buspirone?
This medication is in a category by itself. It is like an SSRI because it specifically targets serotonin receptors (to be exact the 5HT1A receptors) but it also affects dopamine (D2) receptors so it is not completely focused on serotonin.
Notes: Person cannot eat grapefruit or grapefruit juice. Grapefruit juice blocks an enzyme that breaks down the drug. This can increase the drug’s metabolism, causing the strength of the drug to increase by as much as 400%.
If taken with MAO-inhibitors it can cause high blood pressure
How Does Buspirone Work?
- This medication affects neurotransmitter levels, so it may be operating by changing neurons in a way similar to the SSRIs/SNRIs but it also affects dopamine levels.
- The effectiveness of Buspirone in reducing anxiety has not been demonstrated to be effective beyond 3 to 4 weeks.
- Buspirone is often recommended for the treatment of GAD, but there is not much research that provides evidence for its effectiveness
- Because it does not have sedative effects, it has been preferred over benzodiazepines
- There was at least one study that found no ill effects of taking Buspirone for one year
- Because it affects dopamine levels, concerns about Parkinson’s type symptoms has been raised, but nothing beyond a syndrome of restlessness has been reported– and this only in a fraction of cases
|
Beta Blockers
Examples: Propranolol (Inderal), Metoprolol (Lopressor), Atenolol (Tenormin)
How Do They Work?
Beta-blockers keep neurotransmitters like epinephrine (adrenaline) from binding to Beta-adrenergic receptors, keeping adrenaline from having its usual effects of increasing heart rate, etc.
They don’t reduce anxiety but they keep the body from responding with the usual fight-or –flight associated responses.
Taken occasionally, they have almost no side effects
They reduce symptoms of anxiety; are not addictive.
They may interfere with exposure’s effectiveness.
How to explain their Effects to Clients?
They are blocking the body from responding in its usual way to anxiety.
Instead of adrenaline increasing heart rate and other responses like trembling, sweating, flushing, the anxiety stays in the brain and has fewer effects in the body
They can be useful when trembling affects performance or when heart rate increases are distressing to a person.
Note:If a person has been taking them daily, they should not be discontinued abruptly or without medical supervision
Benefits:
Not addictive
Physical symptoms of anxiety are diminished
Helpful in dealing with anxiety sensitivity
Disadvantages/Risks:
Don’t promote client tolerance of anxiety symptoms
Reduce effectiveness of exposure
Side Effects: reduced blood pressure, dizziness, cold hands/feet, tiredness
Physiological Dependence - discontinuation after daily use may increase blood pressure, heart rate
|
Seadatives/Hypnotics/Z-Drugs
Examples: Eszopiclone (Lunesta), Zaleplon (Sonata), Zolpidem (Ambian), Triazolam (Halcion- benzo), Temazepam (Restoril), Diphenhydramine (Benadryl)
How do they work?
Some are benzodiazepines, working by boosting GABA effects.
Z-Drugs, like the benzos, connect to the GABA receptors and open ion channels to polarize the neuron, making it less likely to respond. They are selective for the alpha-1 receptor which promotes sleepiness and doesn’t affect anxiety very much
Antihistamines, especially the older ones, cross the blood/brain barrier and block histamine receptors on neurons that promote wakefulness,. When these neurons are affected, drowsiness occurs.
How to explain their effects to Clients?
Z Drugs are very much like benzodiazepines, boosting GABA effects.
These medications have the effect of inhibiting or sedating neurons, making them less active or putting them to sleep.
They are intended to be used intermittently or for short periods
One can become too reliant on these medications and become unable to sleep without them
Z-Drugs can lose their effectiveness when used regularly
Addiction to Z-drugs can occur after 3-4 weeks and can result in uncomfortable withdrawal symptoms that can last for weeks
Can end up taking z-drugs to prevent withdrawal symptoms, but still not be able to fall asleep
Benefits:
Improve sleep
Disadvantages/Risks:
Addictive
Side Effects: Amnesia, hallucinations, sleepwalking,
Risk of developing depression
Some can cause continuing day-time sedation
Withdrawal reactions, including insomnia, nausea, vomitting
Not recommended for older adults because of risk of falls
Restricted to short-term use not exceeding 2 weeks
Sonata is shortest acting
|
Medications Recommended for Specific Disorders
Phobias: Medications not recommended *CBT
Social Anxiety Disorder: SSRIs (Sertraline, Fluvoxamine, Fluoxetine), SNRIs (Venlafaxine) *CBT or Combined Tx Recommended
Agoraphobia: SSRIs (Sertraline, Fluvoxamine, Fluoxetine), SNRIs (Venlafaxine), *Combined Tx Recommended
Panic Disorder: SSRIs (Paroxetine, Citalopram), SNRIs (Venlafaxine), Tricyclic Antidepressants (Imipramine, Clomipramine)
*Combined Tx Recommended
OCD: SSRIs (Fluvoxamine, Sertraline, Fluoxetine), Tricyclic Antidepressants (Clomipramine), Meds may require extended time for effectiveness *Combined treatment recommended with EX/RP
Generalized Anxiety Disorder: SSRIs (Paroxetine, Fluoxetine), SNRIs (Venlafaxine), Tricyclic Antidepressants (Imipramine, Clomipramine), Buspirone (affects serotonin, dopamine), *Combined Tx Recommended
PTSD: SSRIs (fluoxetine, sertraline), SNRIs (venlafaxine), Meds may require extended time for effectiveness, *Combined Tx Recommended
Note that when benzodiazepines are recommended, it is only for short term use—but in practice this is not followed
Consider Comorbidity Issues
- Tricyclics, SSRIs, SNRIs may be helpful for comorbid depression, which can interfere with participation in treatment.
- Remember that comorbidity is the rule rather than the exception in anxiety disorders, especially with regard to other anxiety disorders, depression, substance misuse.
- When comorbid conditions exist, the use of medications with CBT is recommended
Consider Intensity of Anxiety Symptoms:
- Some clients cannot engage in required daily activities without some relief provided by medication, at least initially (benzodiazepines)
- In disorders where intensity of symptoms varies, use of medication may vary on a daily basis
- Some interventions will increase intensity of symptoms
- In Social Anxiety Disorder and OCD, clients may tolerate exposure treatment only with concurrent treatment with SSRIs/SNRIs or tricyclics
|
Comparing Therapy and Medication in Treating Anxiety Disorders
- Both CBT and pharmacotherapy have demonstrated effectiveness.
- Medications typically cost less than CBT and require less time investment
- Onset of improvement is more rapid with medications
- But, benefits of medication are typically lost with medication discontinuation
- CBT seems to provide more durable effects, with relapse rates lower after CBT
- Pharmacotherapy produces more dropouts – due to side effects
- Clients prefer psychotherapeutic approaches over medication
- No potential for addiction, withdrawal, physical side effects with therapy
- CBT leads to more satisfaction with treatment
- Concerns over medication side effects, dependency, withdrawal, and relapse indicate that CBT should be favored
Anxiety is a Chronic Problem
- Many anxiety disorders have a chronic or recurring course and as a result, short term solutions often do not have the type of effect needed
- When treated as a illness that needs to be cured, there is a tendency to offer medical-model based solutions that manage the problem in the short run, but do not provide durable solutions
- Because medication costs less in the short run than CBT, it is often a preferred method of treatment.
- Unfortunately, some medications provide short term relief but lead to consequences like side effects, addiction, and discontinuation syndromes associated with medication use.
- A client may be expecting results from meds and neglecting therapeutic methods with more lasting effectiveness
Knowing when Meds Might Help
- Although psychiatrists and physicians are the ultimate authority, those who treat anxiety disorders should be familiar with medications frequently used for the disorders they treat
- To know when medications are needed and what medications are most useful for a given disorder enhances the effectiveness and usefulness of a therapist
- With anxiety disorders, use of medication is more complicated than with some other disorders
- Medications are frequently not required for some disorders
- Medication use can be intermittent or situation-based
- Short term impact of medication does not always predict durability
- Medication use may not be coordinated between treating professionals
|
Post Traumatic Stress Disorder
With PTSD the amygdala shrinks – and fires when it shouldn’t & responds to little things
When a trauma occurs it takes 5 hours to change its DNA
Be supportive immediately after a trauma and take them home and have them relax,
If not the DNA does changeand they relive the trauma and the negative change occurs
Major Symptoms
Hypervigilance: Being on guard, jumpy; Exaggerated startle response; irritability/angry outbursts; Nightmares with difficulties getting to and staying asleep
Emotional numbness: Difficulty feeling love and joy & Decreased interest in activities
Avoiding thoughts/situations reminiscent of traumatic events
|
PAIN
Chronic Pain > 3 months
Nociceptive - Signal from Pain Receptor
Nociceptives
SNRIs & Chronic Pain
2 Descending pain modulation pathways (ascending (serotonin) and descending
(norephedrine)); Descend to spinal cord; Inhibit projection of pain information back to brain; Neurons from periaqueductal gray descend to the brain stem nucleus of the raphe and the locus coeruleus; Serotonergic (S) and adrenergic neurons (N), descend to the spinal cord to modulate the transmission of the pain signal
Depression Hurts” – Duloxetine Commercial
5-HT is a NOCICEPTIVE at the level of the dorsal horn (carries sensory information from muscles to skin)
TCAs, SNRIs
Neurokinin 1 & 2 Antagonists (nociceptive)
Possess antidepressant, anxiolytic, anti-emetic properties Discovery was turning point in prevention of N/V associated with cancer chemotherapy
Tachykinin peptide family (NK1, NK2, NK3); Block NK1, ↓ depression (e.g., MK-869)Sub P (NK1), NK2 (NKA) and NK3 (NKB)
Aprepitant/Emend® Used for treatment of CINV – chemically induced nausea/vomiting; • Blocks NK1 receptor in brain stem nuclei of dorsal vagal complex, regulates vomiting
|
|
|