Understanding Pornography: Interventions for Compulsive Users
(An ITTI Training Program)

Module 3: Is Compulsive Use of Pornography an Addiction?
|
|
How Compulsive Pornography Use Mimics Other Addictions in the Brain
|
Is Compulsive Pornography Use an Addiction?
The American Society of Addiction Medicine (ASAM) formally expanded their definition of addiction in 2011 to include both behaviors and substances:
Addiction is a primary, chronic disease of brain reward, motivation, memory and related circuitry. Dysfunction in these circuits leads to characteristic biological, psychological, social and spiritual manifestations. This is reflected in an individual pathologically pursuing reward and/or relief by substance use and other behaviors. There is a Three Stage Model of Addiction which includes:
1.Binge/intoxication
2.Withdrawal/negative affect
3.Preoccupation/anticipation
(Love, et al., 2015)
|
Three Stage Model of Addiction (Love, et al., 2015)
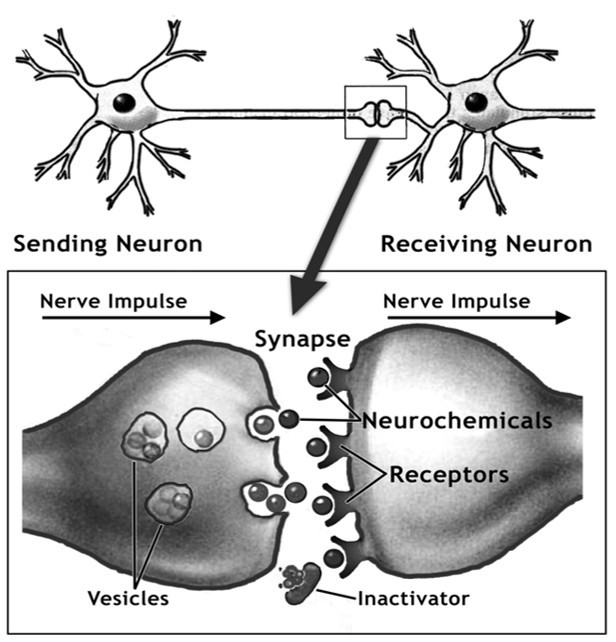
Stage 1: Binge/intoxication
Different classes of drugs activate the reward system through different means, however, the universal result is a flood of dopamine in the Mesolimbic System: Pleasure/Reward Pathways
This results in acute positive reinforcement of the behavior that initiated the flood
In this impulsive stage, this positive reinforcement results in addictive related learning associations
Neuroplastic changes begin to occur, however, as the continued release of dopamine in the Pleasure/Reward Pathways leads to an increase in dynorphin levels
Dynorphin, in turn, decreases the dopaminergic function of the reward system, resulting in a decrease of the reward threshold and an increase in tolerance.
Stage 2: Withdrawal/negative affect
The dopamine flood has run its course, and there is activation of the extended amygdala, an area associated with pain processing and fear conditioning
The resulting negative emotional state leads to activation of brain stress systems and dysregulation of anti-stress systems
This leads to a decreased sensitivity to rewards and an increase in the reward threshold, which is called tolerance
This further progresses to negative reinforcement as the individual continues to engage in the addictive behaviors to avoid the negative affect associated with withdrawal
A second component of the reward system comes into play here: the mesocortical dopamine pathway responsible for key components of cognition and executive function, inhibition & emotional response
Taken together, the mesocortical dopamine pathway affects the cognitive component of reward processing
Stage 3: Preoccupation/anticipation (craving)
The neuroplastic impairments expand beyond the mesocortical dopamine pathway into other regions of the prefrontal cortex responsible for motivation, self-regulation/self-control, delayed reward discounting, and other cognitive and executive functions
This leaves the individual vulnerable to reinstatement of the behavior
Two primary mechanisms have been identified; cue-induced reinstatement and stress induced reinstatement
Numerous neuroimaging studies substantiate this model, and these impairments are the source behind the “chronic relapsing disorder” element of the medical definition of addiction
|
Another take on Porn Addiction
Four characteristics are now associated with the physical changes in brain function as a result of the addiction process. These are:
|
Desensitization: A Numbed Pleasure Response
|
1. Desensitization
‘Desensitization’ is a numbed response to pleasure, especially to natural rewards, like food or bonding with others.
It is usually the first addiction-related brain change porn users notice. They feel depressed, bored, flat and lackluster. Reduced dopamine signaling and other changes leave the heavy user less sensitive to everyday pleasures and ‘hungry’ for dopamine-raising activities and substances. They need greater and greater stimulation to get a buzz.
They may spend more time online, prolonging sessions through edging, watching when not masturbating, or searching for the perfect video to end with.
But desensitization can take the form of escalation to new genres, sometimes harder, stranger, even disturbing. Remember: shock, surprise and anxiety produce adrenaline jack up dopamine and increase sexual arousal.
2. Sensitization
Sensitization triggers powerful cravings or unconscious super-memory of pleasure, ‘euphoric memory’, when activated.
The cue-memory link is the brain that ‘wires together, fires together’ process in action. This conditioned Pavlovian memory makes the addiction more compelling than any other activity in the addict’s life.
The only thing that gets our attention and raises our spirits is the object of our desire, the addicting behavior or substance of choice. This is because we have become very ‘sensitized’ to it
Rewired nerve connections cause the reward system to buzz in response to addiction-related cues or thoughts. Cocaine addicts might see sugar and think of cocaine. An alcoholic hears the clink of glasses or smells beer as he passes a pub and immediately wants to go in.
For the internet porn addict, cues such as turning on the computer, seeing a pop up, or being home alone, trigger intense cravings for porn. Is a guy suddenly much hornier (true libido) when his wife, mother or flatmate goes shopping? Unlikely. But perhaps he feels as if he is on autopilot, or someone else is controlling his brain.
Some describe a sensitized porn response as ‘entering a tunnel that has only one escape: porn’. Maybe he feels a rush, rapid heartbeat, even trembling, and all he can think about is logging onto his favorite porn website. These are examples of sensitized addiction pathways activating the reward system, screaming, “do it now!” Even the risk of committing a sexual offence won’t stop them.
3. Hypofrontality
Hypofrontality, or reduced brain activity in the prefrontal regions, weakens willpower or self-control, in the face of strong subconscious cravings.
This happens as a result of the shrinkage of the grey matter and white matter, in the pre-frontal regions. This is the part of the brain that helps us put the brakes on choices that are not good for our longer-term wellbeing. It helps us say ‘no’ to ourselves when we feel temptation.
With this area depleted, we have a weakened ability to foresee consequences. It can feel like a tug-of-war. The sensitized pathways screaming ‘Yes!’ while the higher brain is saying ‘No! Not again!’
With the executive-control portions of the brain in a weakened condition, the addiction pathway usually wins.
4. Dysfunctional Stress Circuits
Adolescents are doubly vulnerable to addiction. Not only do they have more dopamine driving them to take risks (the accelerator pedal is fully depressed), but the frontal lobes have not fully developed, (the brakes aren’t working too well).
Dysfunctional stress circuits make even minor stress lead to cravings and relapse because they activate powerful sensitized pathways.
These phenomena are at the core of all addictions. One recovering porn addict summed them up: ‘I will never get enough of what doesn’t satisfy me and it never, ever satisfies me’.
Withdrawal. Many people believe that addiction always entails both tolerance (a need for more stimulation to get the same effect, caused by desensitization) and brutal withdrawal symptoms.
In fact, neither is a prerequisite for addiction – although today’s porn users often report both. What all addiction assessment tests share is, continued use despite negative consequences. That is the most reliable evidence of addiction.
|
ICD-11 Diagnosis of Compulsive Sexual Behavior Disorder
In 2017, the World Health Organization adopted a controversial diagnosis as part of the 11th Edition of its International Classification of Disease (ICD-11). Compulsive Sexual Behavior Disorder (CSBD) was established as an Impulse Control Disorder, with the following criteria:
1.Pattern of failure to control intense, sexual impulses or urges and resulting repetitive sexual behavior
2.Manifested over an extended period of time (e.g., 6 months or more)
3.Causes marked distress or significant impairment in personal, family, social, educational, occupational, or other important areas of functioning (distress that is entirely related to moral judgments and disapproval about sexual impulses, urges, or behaviors is not sufficient to meet this requirement)
Caution: Just because some people self-report (after a sexual behavior) that they didn’t feel like they could stop, doesn’t mean they couldn’t stop. Most of these people are actually experiencing regret and remorse for their behaviors, which they reinterpret as a feeling of loss of control. Calling oneself a sex addict is an effective way to externalize the responsibility for one’s choices, as opposed to acknowledging “I made choices that I later wished I hadn’t, because they conflicted with my values, relationship agreements, and religion.” (Ley, 2024)
|
More on ICD-11’s CSBD Diagnosis
An international field study of the ICD-11 CSBD diagnostic criteria reveals that such concerns were likely valid.
Over 1,000 licensed mental health professionals participated in research examining the consistency and accuracy of their diagnostic decisions, utilizing case vignettes and applying criteria from the ICD-11.
The research looked at Compulsive Sexual Behavior Disorder, but also examined criteria and accuracy for gaming disorder, pyromania, kleptomania, and intermittent explosive disorder.
Results for these other disorders were quite positive: Although gaming disorder was controversial and contested, results found that clinicians were largely accurate (79%) when not diagnosing gaming disorder in individuals who gamed frequently but demonstrated no pathological involvement in gaming.
Unfortunately, this was far from true when it came to Compulsive Sexual Behavior Disorder. There, when the vignette described a person who self-identified as a “sex addict,” but demonstrated no evidence of loss of control over their sexual behaviors, fully 50 percent of therapists still diagnosed CSBD, contrary to diagnostic guidelines. (Ley, 2024)
|
References:
Ley, D.J. (2024) The Myth of Sex Addiction. Rowman & Littlefield Publishers ISBN-13978-1442213043
Love, T., Laier, C., Brand, M., Hatch, L. & Hajela, R. (2015). Neuroscience of internet pornography addiction: A review and update. Behavioral Science, 5, 388-433. doi:10.3390/bs5030388
|
|
|