Pain Management -
A Neurobiological Approach
|
|
Mindfulness & Neurobiological
Tools for Healing - A Training Resource
By Jim Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
The Take Aways from the Pain Management Best Practices
On May 9, 2019, the Pain Management Best Practices Inter-Agency Task Force under the watchful eye of the U.S. Department of Health and Human Services published its Report: Pain Management Best Practices. The report included the following sections: Clinical Best Practices for Pain Management including 1. Medications; 2. Restorative Therapies; 3. Interventional Procedures; 4. Behavioral Health Approaches and 5. Complementary and Integrative Health.
Significantly for this work MBSR (Mindfulness Based Stress Reduction) was listed not only in the Behavioral Health Approaches but also in the Complementary and Integrative Health Best Clinical Practices.
This report points out that MBSR is a mind-body treatment typically delivered in a group format. MBSR focuses on improving patients' awareness and acceptance of their physical and psychological experiences through body awareness and intensive training in mindfulness meditation (HHS, 2019, p. 38).
This report points out that MBSR teaches patients to self-regulate their pain and pain-related comorbidities by developing nonjudgmental awareness and acceptance of present-moment sensations, emotions, and thoughts (HHS, 2019, p. 38).
This report points out that research on MBSR points out its effectiveness in helping individuals cope with a variety of paiin conditions including rheumatoid arthritis, low back pain, and MS. Also, that MBSR has a positive impact on pain intensity, sleep quality, fatigue, and overall physical functioning and well being (HHS, 2019, p. 38).
In this report under Complementaruy and Integrative Healthy Approaches, it points out that MBSR incorporates mindfulness skills training to enhance one's ability to manage or reduce pain. Mindfulness enables an attentional stance of removed observation and is characterized by concentrating on the present moment with openness, curiosity and acceptance, allowing for changes in one's point of view on the pain experieince. In this section of the report it points out that MBSR significantly reduces the intensity and frequency of primary heachache pain, and has significant benefits for low-back pain. (HHS, 2019, p. 43).
Reference:
|
Pain Management Overview
Pain management is important for ongoing pain control, especially if you suffer with long-term or chronic pain. After getting a pain assessment, your doctor can prescribe pain medicine, other pain treatments, or psychotherapy to help with pain relief.
Chronic Pain
Of the 50 million Americans living with chronic pain, the pain is so bad for 20 million that it keeps them from doing the daily activities of life, researchers say. According to a report from the U.S. Centers for Disease Control and Prevention, chronic pain and high-impact chronic pain are more common among women, older adults, the poor, people previously employed, those with public health insurance or living in rural areas.Not only is chronic pain widespread, it lies at the root of the opioid epidemic.
|
Assessment of Pain
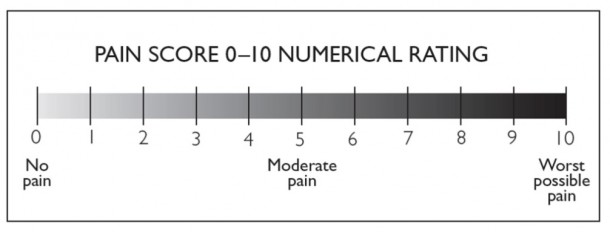
Numeric Pain Rating Scale
SOAPP (Screener and Opioid Risk Assessment for Patients with Pain) and COOM (Current Opioid Misue Measure are both available from PainEdu at: https://www.painedu.org/
|
Non-Medication Pain Management Review of the Literature
Overview of Non-Medication Approaches to Pain Management
Patient expectations may be associated with outcomes of complementary and alternative medicine (CAM) treatments for chronic pain and a psychometrically sound measure of such expectations called the EXPECT Questionnaire has been researched and is now available for use (Jones et al., 2016). You can view the original article and EXPECT at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5116692/
A study in 2016 was done to analyze the factors which are barriers to patients’ utilization of non-medication therapeutic approaches to chronic pain. This study found that Patients on long-term opioid therapy report using multiple types of pain treatments. High rates of complementary and alternative medicines (CAM) use were impacted by the limited evidence of efficacy for some therapies and the low-income status of most people with chronic non-cancer pain. Financial and insurance barriers highlighted the importance of considering how different types of treatments are paid for and subsidized (Nielsen et al., 2016). The use of alternative or non-medication solutions to chronic pain must always include in their consideration how the costs of such services will be handled by the target patients.
In talking about pain management, it is important for those who work with these patients to remember providing support in relation to the diagnostic label rather than to individual patient experiences; ‘pain as pathology’ rather than ‘pain in the patient’ does not always help the patients in pain (Sanders et al., 2015). It is important that in helping patients with pain that we focus on them since pain does alter their definition and understanding of themselves.
When considering patient variables, it was found that Mindfulness meditation makes a difference for patients. Patients felt rested and were in better control of their pain and its role in their life. Patients who recognized that pain is part of their life and were living under stable conditions may have been more likely to learn and put forth personal effort, which may have made change possible (Petersen & La Cour, 2016). A 2017 study found that the majority of patients using complementary and alternative medicine (CAM) perceived benefits in particular, women living in urban areas, highly educated, aged more than 40, who suffer from severe chronic back pain (Kavadar et al., 2017)
When patients were asked about their experience in the VA and their opinions about which therapies would most benefit other Veterans. Participants reported that massage was well-received and resulted in decreased pain, increased mobility, and decreased opioid use but there were factors which often impeded their ability to acquire such services such as high ration of patients to complementary and integrative health(CIH) providers, difficulty of ability of receiving CIH from fee-based CIH providers outside of the VA, cost issues (Fletcher et al., 2016). The cost of CIH in the community is an important factor which must be closely watched in helping patients to acquire non-medication approached to chronic pain.
In 2008, 83 studies were included, comprising the following subjects: exercise therapy back schools, TENS, low-level laser therapy, massage, behavioral treatment, patient education, traction, and multidisciplinary treatment. This review showed that behavioral therapy had an effect on pain intensity. This is apparent because the aim of behavioral therapy is not to treat pain, but to modify one of the three response systems (behavioral, cognition, and physiological reactivity). This study concluded that decrease in pain intensity might be related to the combination of different treatment strategies applied in a great number of the included studies (van Middelkoop et al., 2011). It has been found that use of exercises only is noninvasive, non-pharmaceutical and an effective method to reduce knee pain in patients with knee osteoarthritis (Jaskiran et al., 2015).
A systematic meta-analysis of 42 studies in behavioral non-medication intervention (Including Mindfulness-Based Stress Reduction (MBSR) Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT) with patients with chronic low back pain (LBP), it was found that behavioral therapy approaches are: 1. Effective particularly in altering pain perception and helping patients to regain their functionality. 2. Treatment outcomes can be improved if the treatments are personalized to individual patients’ needs. 3. Multidisciplinary rehabilitation needs to include more than just physical treatment. A team approach accounting for several aspects within the bio-psychosocial model is more likely to help individuals with chronic LBP compared to standard care alone (Vitoula et al. 2017).
An innovative approach to help patients deal with delayed-onset muscle soreness (DOMS) The use of herbs in DOMS seems safer and has lower side effects than pharmacotherapy (Meamarbashi, 2017).
In 2018 in an article in the Journal of Family Practice a report on a meta-analytic review of 42 articles on non-medication pain management the conclusion was that a pain management plan needs to include the following non-medication modalities recommendations:
1. Self-care goals2. Exercise or movement-based treatments (e.g. Therapeutic exercise, yoga, tai chi)3. Mind-body treatment (e.g. Mindfulness, Mindful cognitive behavioral therapy, biofeedback)4. Complementary modalities (e.g. Physical therapy, osteopathic manipulative treatment, chiropractic, massage) (Lemmon & Hamptom, 2018) at: https://www.mdedge.com/jfponline/article/170928/pain/nonpharmacologic-treatment-chronic-pain-what-works
Overview Section Summary:
The research literature, for non-medication treatment of chronic pain, points out specific issues which must be addressed in setting up such a treatment model:Evidence supports the need for any proposed model of non-medication treatment for chronic pain must include all of the following components:
1. Training of patients in self-care including: eating healthy nutritionally balanced meals, participating in a detailed exercise program including aerobic and stretching routines, and maintaining a healthy regimen of 7-8 hours of sleep nightly.
2. Specialized movement programming be it yoga, tai chi or specific stretching and strength exercise modalities coached by a trained professional.
3. Individual or group Psychotherapy using a Mindfulness based program such as MBSR, MBCBT and ACT.
4. Specialized complementary modalities such as massage, physical therapy or other osteopathic or chiropractic manipulative treatments.
5. Evidence show that patients will be more successful in efforts to help them manage their chronic pain without medications if they have a positive expectation about the program of non-medication they will be going through and if they have a clear understanding of the potential length of time their treatment will take.
6. To assist patients to have more positive expectations about their non-medication treatment for chronic pain it is important that they be provided psycho-education about the research support for the use of the interventions to be used and that the costs of such interventions are either supported by their insurance health plans or are at a reasonable enough cost not to put a strain on their personal finances.
7. That proposed models of non-medication treatment for chronic pain focus their attention on the patients’ feelings, emotional supports, full understanding of the strategies involved in such treatment and feel that they are being treated as a “person” rather than a “pain diagnosed subject.”
The anticipated models for non-medication treatment of chronic pain must have Mindfulness at its foundation and that all professionals involved on the treatment team are supportive, informed and collaborate with the patients in the use of mindfulness in their respective portion of their planned treatment for the patients.
|
References
Overview of Non-Medication Approaches to Pain Management
Jaskiran, K., Anil, K. & Chandanpreet, K. (2015). Effectiveness of exercises therapy on pain among patients with knee osteoarthritis. Baba Farid University Nursing Journal,8(1), 34-37.
Jones, S.M.W., Lange, J., Turner, J., Cherkin, D., Ritenbaugh, C., Hsu, C., Berthoud, H. & Sherman, K. (2016). Development and validation of the EXPECT questionnaire: Assessing patient expectations of outcomes of complementary and alternative medicine treatments for chronic pain. The Journal of Alternative and Complementary Medicine, 22(11), 936-946. DOI: 10.1089/acm.2016.0242
Kavadar, G., Demircioglu, D.T., Can, H., Emre, T.Y., Civelek, E. & Senyigit, A. (2017). The clinical factors associated with benefit finding of complementary medicine use in patients with back pain: A cross-sectional study with cluster analysis. Journal of Back and Musculoskeletal Rehabilitation, 30, 271-277. DOI 10.3233/BMR-150470
Lemmon, R. & Hampton, A. (2018). Nonpharmacologic treatment of chronic pain: What works? The Journal of Family Practice, 67(8), 474-483.
Meamarbashi, A. (2017). Herbs and natural supplements in the prevention and treatment of delayed-onset muscle soreness. Avicenna Journal of Phytomedicine (AJP), 7(1), 16-26.
Nielson, S., Campbell, G., Peacock, A., Smith, K., Bruno, R., Hall, W., Cohen, M. & Degenhardt, L. (2016). Health service utilisation by people living with chronic non-cancer pain: findings from the Pain and Opioids in Treatment (POINT) study. Australian Health Review, 40, 490-499. http://dx.doi.org/10.1071/AH15047
Sanders, T., Ong, B.N., Roberts, D. & Cotbett, M. (2015). Health maintenance, meaning, and disrupted illness trajectories in people with low back pain: a qualitative study. Health Sociology Review, 24(1), 1-14. http://dx.doi.org/10.1080/14461242.2014.999399
Van Middelkoop, M., Rubinstenin, S.M., Kinjpers, T., Verhagen, A.P., Ostelo, R., Koes, B.W. & Van Tulder, M.W. (2011). A systematic review on the effectiveness of physical and rehabilitation interventions for chronic non-specific low back pain. European Spine Journal 20,19-39. DOI 10.1007/s00586-010-1518-3
|
Mindfulness-Based Interventions for Chronic Pain
A preliminary Systematic review of the literature in 2011 found that studies up to that date showed that Mindfulness Based Interventions (IBIs) could have nonspecific effects for the reduction of pain symptoms and the improvement of depressive symptoms in patients with chronic pain as well as some improvements in psychologic measures related to chronic pain such as copying with pain following MBIs (Chiesa & Serretti, 2011). In 2017 another meta-analysis of 38 studies found that mindfulness meditation was associated with decrease in pain, reduction of depressive symptoms and increase in quality of life (Hilton et al., 2017). An analysis of the mechanisms impacted by Mindfulness meditation demonstrated its effectiveness in reducing pain through multiple unique physiological mechanisms (Zeiden & Vago, 2016). Mindfulness was also found to be a useful intervention for the management of post stroke Neuropathic Pain when used independently of other intervention components (Brown & Becerra, 2017)
Ongoing research has supported the benefits of mindfulness intervention on chronic pain (Howarth et al., 2016; Dunkley & Brotto, 2016; Poulin et al., 2016; Grazzi et al., 2017)
There has been a movement to combine Mindfulness not only with Stress Reduction for treating pain but also to combine Mindfulness with both Acceptance and Commitment Therapy (ACT) and Existential Therapy to better focus patient with pain on personal empowerment in the face of unpleasant aspects of the human condition (Harris, 2013). Again, Acceptance and Commitment Therapy (ACT) and Mindfulness were presented as an ideal model for treating chronic pain (McCarcken & Vowles, 2014).
A meta-analytic review of twenty-five Randomly Controlled Studies (RCT totaling 1285 patients with chronic pain, compared acceptance- and mindfulness-based interventions to the waitlist, (medical) treatment-as-usual, and education or support control groups. Outcome measures were pain intensity, depression, anxiety, pain interference, disability and quality of life. ACT showed significantly higher effects on depression and anxiety than MBSR and MBCT (Veehof et al., 2016). Mindfulness strategies applied in vocational rehabilitation practice settings helped workers with chronic pain achieve job satisfaction, job satisfactoriness, job retention, and high levels of quality of life (Davenport et al., 2017)
Strong encouragement has been made to utilize Mindfulness-Based Stress Reduction (MBSR) with patients with chronic pain because it focuses not only on the mind but also the body, it has the potential to address some of the psychosocial factors that are important predictors of poor outcomes (Cherkin et al., 2014). Also, MBSR was found to contribute positively to pain management by lowering anxiety and depression, feelings of controlling pain and acceptance of higher pain which are important dimensions in patients with long-lasting chronic pain (la Cour & Petersen, 2015). MBSR was also found that patients revealed significant and clinically relevant improvements in level of pain disability, psychological distress, engagement in life activities, willingness to experience pain and subjective ratings of their current pain (Beaulac & Bailly, 2015). Use of MBSR with women with chronic pelvic pain has shown promise in pain reduction (Crisp et al., 2016). Use of MBSR with chronic low pain demonstrated through the measurement of increase in quality of life and decrease in pain severity (Ardito et al., 2017). MBSR was used with patients with painful diabetic peripheral neuropathy resulting in reduced pain intensity, pain catastrophizing, depression, perceived stress and improved health related quality of life (Nathan et al.,2017).
In treating Irritable bowel syndrome (IBS) characterized by abdominal pain and hypervigilance to gastrointestinal sensations Mindfulness Treatment appeared to target and ameliorate the underlying pathogenic mechanisms of IBS (Garland et al, 2012).
Mindfulness-Based Cognitive Therapy (MBCT) and Second Generation Mindfulness Based Intervention (SG-MBI) were both found to reduce the impact of fibromyalgia, its depressive symptoms and intensity of pain (Parra-Delgado & Latorre-Postigo, 2013; Van Gorden et al., 2017).
Participants with chronic pain in a Mindfulness-Oriented Recovery Enhancement (MORE) 8-week program were found after a three month follow up study to have improvement in general activity level and walking ability (Garland et al., 2014). In working with patients with chronic pain who are opioid seeking would benefit from the MORE process through its cognitive training regimens centered on strengthening attention to natural rewards may remediate reward processing deficits underpinning addictive behavior (Garland et al., 2015).
In a systematic review of 23 studies using MBSR and MBCT There was found improved depressive symptoms, anxiety, stress, quality of life and physical functioning. The evidence supports the use of MBSR and MBCT to alleviate symptoms, both mental and physical, in the adjunct treatment of cancer, cardiovascular disease, chronic pain, depression, anxiety disorders and in prevention in healthy adults and children (Gotink et al., 2015). Pain catastrophizing and psychological distress were identified as individual mediators of the relationship between mindfulness and depressive symptoms for people with chronic pain thus supporting the inclusion of the use of mindfulness based cognitive interventions with these individual (Brooks et al., 2018).
A Web-based Mindfulness 8-week training program on pain intensity, pain acceptance and life satisfaction was demonstrated as being reasonably successful and open for future research and replication (Henriksson, Wasara & Ronnlund, 2016).
Mindfulness Section Summary
1. Counseling which is mindfulness based be provided individually or in group to address the cognitive, emotional and behavioral coping with pain but also to address specifically the lessening of catastrophizing, stress, depression, anxiety and any other psychological distress and increase in self-esteem, and quality of life.
2. That MBSR, MBCT, MBACT treatment modalities be the psychotherapeutic treatments used with these patients with chronic pain due to their receiving the strongest research support for their effectiveness.
3. That the psychotherapeutic mindfulness models can be time limited, not just provided soley in person individually and in group but also supported by the use of Apps, Podcasts, Videos and Web-based programming.
|
References
Mindfulness-Based Interventions for Chronic Pain
Ardito, R.B., Pirro, P.S., Re, T.S., Bonapace, I., Bruno, E. & Gianotti, L. (2017). Mindfulness-based stress reduction program on chronic low-back pain: A study investigating the impact on endocrine, physical, and psychologic functioning. The Journal of Alternative and Complementary Medicine, 23(8), 615-623. DOI: 10.1089/acm.2016.0423
Beaulac, J. & Bailly, M. (2015). Mindfulness-based stress reduction: Pilot study of a treatment group for patients with chronic pain in a primary care setting. Primary Health Care Research & Development, 16(4), 424-428. DOI: 10.1017/S1463423614000346
Brooks, J.M. Blake, J., Iwanaga, K., Chin, C., Colton, B.P., Morrison, B., Deiches, J. & Chan, F. (2018). Perceived mindfulness and depressive symptoms among people with chronic pain. Journal of Rehabilitation 84 (2), 33-39.
Brown, A. & Becerra, R. (2017). Mindfulness for neuropathic pain: A case study. International Journal of Psychology and Psychological Therapy, 17(1)19-37.
Cherkin, D.C., Serman, K.J., Balderson, B.H., Turner, J.A., Cook, A.J., Stoelb, B., Herman, P.M., Deyo, R.A. & Hawkes, R.J. (2014). Comparison of complementary and alternative medicine with conventional mind-body therapies for chronic back pain: Protocol for the mind-body approaches to pain (MAP) randomized controlled trial. Trials, 15, 211. doi:10.1186/1745-6215-15-211
Chiesa, A. & Serreti, A. (2011). Mindfulness-based interventions for chronic pain: A systematic review of the evidence. The Journal of Alternative and Complementary Medicine, 17(1), 83-89.
Crisp, C.D., Hastings-Tolsma, M. & Jonscher, K.R. (2016). Mindfulness-based stress reduction for military women with chronic pelvic pain: A feasibility study. Military Medicine, 181(9), 982-989.
Davenport, J., Koch, L.C. & Rumrill, P.D. (2017). Mindfulness-based approaches for managing chronic pain: Applications to vocational rehabilitation and employment. Journal of Vocational Rehabilitation 47, 247–258. DOI:10.3233/JVR-170899
Dunkley, C.R. & Brotto, L.A. (2016). Psychological treatments for provoked vestibulodynia: Integration of mindfulness-based and cognitive behavioral therapies. Journal of Clinical Psychology, 72(7), 637-650. DOI: 10.1002/jclp.22286
Garland, E.L., Froeliger, B. & Howard, M.O. (2015). Neurophysiological evidence for remediation of reward processing deficits in chronic pain and opioid misuse following treatment with Mindfulness-Oriented Recovery Enhancement: exploratory ERP findings from a pilot RCT. Journal of Behavioral Medicine, 38, 327-336. DOI 10.1007/s10865-014-9607-0
Garland, E.L. Gaylord, S.A., Palsson, O., Faurot, K., Mann, J.D. & Whitehead, W.F. (2012). Therapeutic mechanisms of a mindfulness-based treatment for IBS: Effects on visceral sensitivity, catastrophizing, and affective processing of pain sensations. Journal of Behavioral Medicine, 35. 591-602. DOI 10.1007/s10865-011-9391-z
Garland, E.L, Thomas, E. & Howard, M.O. (2014). Mindfulness-oriented recovery enhancement ameliorates the impact of pain on self-reported psychological and physical function among opioid-using Chronic pain patients. Journal of Pain and Symptom Management 48(6) 1091-1098.
Gotink, R.A., Chu, P., Busschbach, J.J.V., Benson, H., Fricchione, L. & Hunink, M.G.M. (2015). Standardized mindfulness-based interventions in healthcare: An overview of systematic reviews and meta-analyses of RCTs. PLoS ONE,10(4), 1-17. DOI:10.1371/journal.pone.0124344
Grazzi, L., D’Amico, D., Raggi, A., Leonardi, M., Ciusani, E., Corsini, E, D’Andrea, G., Bolner, A., Salgado-Garcia, F., Andrasik, F. & Sansone, E. (2017). Mindfulness and pharmacological prophylaxis have comparable effect on biomarkers of inflammation and clinical indexes in chronic migraine with medication overuse: Results at 12 months after withdrawal. Neurological Science 38, S173-S175. DOI 10.1007/s10072-017-2874-0
Harris, W. (2013). Mindfulness-based existential therapy: Connecting mindfulness and existential therapy. Journal of Creativity in Mental Health, 8, 349–362. DOI: 10.1080/15401383.2013.844655
Henricksson, J., Wasara, E. & Ronnlund, M. (2016). Effects of eight-week- web-based mindfulness training on pain intensity, pain acceptance, and life satisfaction in individuals with chronic pain. Psychological Reports, 119(3), 586-607. DOI: 10.1177/0033294116675086
Hilton, L., Hempel, S., Ewing, B.A., Apaydin, E., Xenakis, L., Newberry, S., Colaiaco, B., Maher, A.R., Shanman, R. M., Sorbero, M.E. & Maglione, M.A. (2017). Mindfulness meditation for chronic pain: Systematic review and meta-analysis. Annals of Behavioral Medicine, 51, 199-213. DOI 10.1007/s12160-016-9844-2
Howarth, A., Perkins-Porres, L., Smith, J.G., Subramaniam, J., Copland, C., Hurley, M., Beith, I., Riaz, M. & Ussher, M. (2016). Pilot study evaluating a brief mindfulness intervention for those with chronic pain: Study protocol for a randomized controlled trial. Trial, 17, 273. DOI 10.1186/s13063-016-1405-2
La Cour, P. & Petersen, M. (2015). Effects of mindfulness meditation on chronic pain: A randomized controlled trial, Pain Medicine, 16. 641-652.
McCracken, L.M. & Vowles, K.E. (2014). Acceptance and commitment therapy and mindfulness for chronic pain: Model, process and progress. American Psychologist, 69(2), 178-187. DOI: 10.1037/a0035623
Nathan, H.J., Poulin, P., Wozny, D., Taljaard, M., Smyth, C., Gilron, I., Sorisky, A., Lochnan, H. & Shergill, Y. (2017), Randomized trial of the effect of mindfulness-based stress reduction on pain-related disability, pain intensity, health-related quality of life, and A1C in patients with painful diabetic peripheral neuropathy. Clinical Diabetes Journals 35/5/294. DOI: 10.2337/cd17-0077
Parra-Delgado, M. & Latorre-Postigo, J.M. (2013). Effectiveness of mindfulness-based cognitive therapy in the treatment of dibromyalgia: A randomised trial. Cognitive Therapy and Research, 37, 1015-1026. DOI 10.1007/s10608-013-9538-z
Petersen, M. & La Cour, P. (2016). Mindfulness—what works for whom? Referral, feasibility, and user perspectives regarding patients with mixed chronic pain. The Journal of Alternative and Complementary Medicine, 22(4), 298-305. DOI: 10.1089/acm.2015.0310
Poulin, P.A., Romanow, H.C., Rahbari, N., Small, R., Smyth, C.E., Hatchard, T., Solomon, B.K., Song, X., Harris, C.A., Kowal, J., Nathan, H.J. & Wilson, K.G. (2016). The relationship between mindfulness, pain intensity, pain catastrophizing, depression, and quality of life among cancer survivors living with chronic neuropathic pain. Support Care Cancer, 24. 4167-4175. DOI 10.1007/s00520-016-3243-x
Veehof, M.M., Trompetter, H.R., Bohlmeijer, E.T. & Schreurs, K.M.G. (2016). Acceptance- and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cognitive Behaviour Therapy, 45(1), 5-31. http://dx.doi.org/10.1080/16506073.2015.1098724
Van Gorden, W., Shonin, E., Dunn, T.J., Garcia-Campayo, J. & Griffiths, M.D. (2017). Meditation awareness training for the treatment of fibromyalgia syndrome: A randomized controlled trial. British Journal of Health Psychology, 22, 186-206. DOI:10.1111/bjhp.12224
Vitoula, K., Venneri, A., Verrassi, G., Paladini, A., Sykioti, P., Adewusi, J. & Zis, P. (2017). Behavioral therapy approaches for the management of low back pain: An up-to-date systematic review. Pain Therapy, 7,1–12. https://doi.org/10.1007/s40122-018-0099-4
Zeidan, F. & Vago, D.R. (2016). Mindfulness meditation-based relief: A mechanistic account. Annals of the New York Academy of Sciences 1373, 114-127. doi: 10.1111/nyas.13153
|
Massage Therapy for Pain Management
Boylan (2005) was one of the first researchers to report that soft tissue massage may be of clinical assistance to patients with shoulder pain, especially for patients awaiting additional treatment. In 2011 a study demonstrated that patients who received exercise only or exercise with transverse friction massage (TFM) prior to exercise and the TFM group improved best in terms of pain/function (Blackwood & Ghazi, 2012). Functional Massage (FM) is a therapeutic technique that incorporates joint motion with massage to treat musculotendinous pain and impairments was found to reduce the report of pain and increase the range of motion for patients (Sobeck, et al., 2016).
After reviewing 20 studies of the use of soft tissue massage and exercise in the treatment of non-specific shoulder pain it was found that there is low-quality evidence that soft tissue massage is effective for improving pain, function and range of motion in patients with shoulder pain in the short term. Exercise therapy was found to be effective for producing small improvements in pain but not in function or range of motion (van den Dolder, Ferreira & Refshauge, 2014). In a live trial the findings from their 2014 report found that the addition of soft tissue massage to an exercise program for the shoulder conferred no additional benefit for improving pain, disability, or range of motion in people with nonspecific shoulder pain (van den Dolder, Ferreira & Refshauge, 2015).
A meta-analysis of twelve research studies on Massage Therapy (MT) for neck and shoulder pain were performed. The findings were that MT provides immediate effects for neck and shoulder pain. However, MT did not show better effects on pain than other active therapies. Nor did evidence suggest that MT was effective in improving functional status (Kong, et al. 2013). In 2014 researchers found that patients seeking massage for chronic neck pain are more likely to benefit if they have multiple 60-minute treatments per week (Sherman, et al, 2014). Research has shown that massage in treating neck pain is effective, efficient, and safe (Skillgate, Bill, Cote, Viklund, Peterson & Holm, 2015). Effective massage treatment with progressive sessions which allow the client to practice self-help exercises or other home treatments (ice or hot/cold contrast) that Help expedite recovery for neck pain helps return clients to a more active, pain free lifestyle (Kousaleos, 2015).
Patients with spinal cord injuries during their acute rehabilitation were either given broad compression massage (BCM) and a control light contact touch (LCT) treatment and it was found that BCM was safe and well tolerated and ought to continue to be utilized (Chase, Jha, Brooks & Allshouse, 2013).
Patients experiencing generalize physical pain while in hospital received massage and indicated satisfaction with their treatment and experienced a reduction in pain intensity, a significant increase in daily function and reduction in anxiety (McMillan, Glaser & Radovich, 2018).
Massage Therapy and Abdominal Hypopressive Gymnastics and the combination of both was used to decrease pain and lumbar disability while increasing joint mobility and quality of life in patients with chronic nonspecific low back pain experienced reduced pain levels, improved disability, and increased t flexibility of the lumbar spine (Bellido-Fernandez, et al., 2018)
Use of massage versus traditional physical therapy was studied with patients with low back pain and it was found that both massage therapy and routine physical therapy are useful for sub-acute and chronic nonspecific low back pain treatment especially if accompanied with exercise (Kamali, Panahi, Ebrahimin & Abbasi, 2014). A study concluded that there are arrays of conservative treatments shown to be effective in treating Lower Back Pain (LBP), however, massage and spinal manipulation are the most popular among LBP patients because it contributes good effect in reducing pain intensity (Sejari, Kamaruddin, Al-Worafi & Ming, 2014). The efficacy of massage and for chronic low back pain in “real-world” primary health care was shown to have major impact on pain, disability, and health-related quality of life for primary care patients with chronic low back pain (Elder, Munk, Love, Bruckner, Stewart & Pearce, 2017)
Research in to manual therapy as spinal manipulation, spinal mobilization, stretching and massage are common treatment methods for neck and back pain found that they were effective in reducing the pain in the patients followed in a one year follow-up study (Paanalahti, et al., 2016). Both Deep Tissue Massage (DTM) and Therapeutic Massage (TM) were found to provide to provide clinical benefits to individuals with chronic back pain (Romanowski, 2017).
Massage Section Summary:
Massage as the sole treatment for chronic pain is not research supported, however it is greatly supported to be part of a comprehensive multidisciplinary approach of non-medication treatment for chronic pain.
|
References
Massage
Bellido-Fernandez, L., Jimenez-Rejano, J.J., Chillon-Martinez, R., Gomez-Benitex, M.A., De-La-Casa-Almeida, M. & Rebollo-Salas, M. (2018). Effectiveness of massage therapy and abdominal hypopressive gymnastics in nonspecific chronic low back pain: A randomized controlled pilot study. Evidence-Based Complementary and Alternative Medicine 2018, Article ID 3684194, 9 pages. https://doi.org/10.1155/2018/3684194
Blackwood, J. & Ghazi, F. (2012). Can the addition of transverse friction massage to an exercise programme in treatment of infrapatellar tendinopathy reduce pain and function? A pilot study. International Musculoskeletal Medicine, 34(3). 108-114.
Boylan, M. (2005). Soft tissue massage improves range of motion, function and pain in shoulder pain. Journal of Australian Traditional Medical Society11(4), 177-178.
Chase, T., Jha, A., Brooks, C.A. & Allshouse, A. (2013) A pilot feasibility study of massage to reduce pain in people with spinal cord injury during acute rehabilitation. Spinal Cord, 51,847-851.
Elder, W.G., Munk, N., Love, M.M., Bruckner, G.G., Stewart, K.E. & Pearce, K. (2017). Real-world massage therapy produces meaningful effectiveness signal for primary care patients with chronic low back pain: Results of a repeated measures cohort study. Pain Medicine, 18, 1394-1405. doi: 10.1093/pm/pnw347
Fletcher, C.E., Mitchinson, A.R., Trumble, E.I., Hinshaw, D.B. & Dusek, J.A. (2016). Perceptions of other integrative health therapies by veterans with pain who are receiving massage. JRRD, 53(1), 117-126. http://dx.doi.org/10.1682/JRRD.2015.01.0015
Kamali, F., Panahi, F., Ebrahimin, S. & Abbasi, L. (2014). Comparison between massage and routine physical therapy in women with sub acute and chronic nonspecific low back pain. Journal of Back and Musculoskeletal Rehabilitation,27475-480. DOI 10.3233/BMR-140468
Kong, L.J., Zhan,H.S., Cheng,Y.U. Yuan,W,A., Chen, B. & Fang, M. (2013). Massage therapy for neck and shoulder pain: A systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine, 2013. Article ID 6133279, http://dx.doi.org/10.1155/2013/613279
Kousaleos, G.P. (2015). Neck pain and treatment strategies. Journal of the Australian Traditional-Medicine Society, 21(1), 16-21.
McMillan, K., Glaser, D. & Radovich, P. (2018). The effect of massage on pain and anxiety in hospitalized patients: An observational study. MEDSURG Nursing, 27(1), 14-18.
Paanalahti, K., Holm, L.W., Nordin, M., Hoijer, J., Lyander, J., Asker, & Skillgate, E, (2016). Three combinations of manual therapy techniques within naprapathy in the treatment of neck and/or back pain: a randomized controlled trial. BMC Musculoskeletal Disorders, 17, 176. DOI 10.1186/s12891-016-1030-y
Romanowski, M.W., Spiritovic, M., Rukowski, R., Dudek, A., Samborski, W. & Straburzynska-Lupa, A. (2017). Comparison of deep tissue massage and therapeutic massage for lower back pain, disease activity, and functional capacity of ankylosing spondylitis patients: A randomized clinical pilot study. Evidence-Based Complementary and Alternative Medicine, 2017, 7 pages. https://doi.org/10.1155/2017/9894128
Sejari, N., Kamaruddin, K., Al-Warafi Y.M.A. & Ming, L.C. (2014). A narrative review of massage and spinal manipulation in the treatment of low back pain. Archives of Pharmacy Practice, 5(4), 139-143.
Sherman, K.J., Cook, A.J., Wellman, R.D., Hawkes, R.J., Kahn, J.R., Deyo, R. A. & Cherkin, D.C. (2014). Five-week outcomes from a dosing trial of therapeutic massage for chronic neck pain. Annals of Family Medicine, 12(2),
Skillgate, E., Bill, A.S., Cote, P, Viklund, P., Peterson, A. & Holm, L.W. (2015). The effect of massage therapy and/or exercise therapy on subacute or long-lasting neck pain - The Stockholm Neck Trial (STONE): study protocol for a randomized controlled trial. Trials,16,414 DOI10.1186/s13063-015-0926-4
Sobeck, C., Lenk, L., Knipper, S., Rhoda, A., Stickler, L. & Stephenson, P. (2016). The effectiveness of functional massage on pain and range of motion measurements in patients with orthopedic impairments of the extremities. International Musculoskeletal Medicine 38(1), 21-25. DOI 10.1080/17536146.2016.1173342
van den Dolder, P.A., Ferreira, P.H. & Refshauge, K.M. (2014). Effectiveness of soft tissue massage and exercise for the treatment of non-specific shoulder pain: A systematic review with meta-analysis. Journal of Sports Medicine,48, 1216-1226. doi:10.1136/bjsports-2011-090553
van den Dolder, P.A., Ferreira, P.H. & Refshauge, K.M. (2015). Effectiveness of soft tissue massage for nonspecific shoulder pain: Randomized controlled Trial. Physical Therapy, 95(11), 1467-1477.
|
Yoga for Pain Management
A study demonstrated that a 9-week yoga intervention improved pain and neck-related disability for at least 12 months after completion and that sustained yoga practice seems to be the most important predictor of long-term effectiveness (Cramer, Lauche, Hohmann, Langhorst & Dobos, 2013). Another study found that yoga and relaxation techniques are a better and beneficial therapy in the treatment of pain and stiffness of the neck region (Satyanand, et al., 2015). Yoga twice a week was found to reduce absenteeism for those with non-specific back pain and neck pain (Bramberg, Bergstrom, Jensen, Hagberg & Kwak, 2017).
A study on the impact of yoga on non-specific low back pain (nsLBP) and sciatica found that yoga therapy can be safe and beneficial for patients with nsLBP or sciatica, accompanied by disc extrusions and bulges (Monro, Bhardwaj, Gupta, Telles, Allen & Little, 2015). Yoga has be identified as an effective treatment for Veterans with chronic low back pain and psychological comorbidities (Saper, et al., 2017).
Yoga and walking when used with patients with Irritable bowel syndrome (IBS) as movement-based self-regulatory behavioral treatments have some differential and beneficial effects but maintenance of a self-regulated walking program may be more feasible and therefore more effective in the long term (Shahabi, Naliboff & Shapiro, 2016).
A study found that yoga-based intervention can be one of the non-pharmacological treatment options in somatoform disorders (Sutar, Yadav & Desai, 2016), Yoga twice a week was found to assist trainees to focus on their specific professional training with no concern for musculoskeletal pain (Monson, Chismark, Cooper & Krenik-Matejcek, 2017). Yoga practice was associated with a reduction in levels of chronic pelvic pain and an improvement in Quality of Life in women with endometriosis (Goncalves, Barros & Behamondes, 2017).
Yoga Section Summary:
Yoga as the sole treatment for chronic pain is not research supported, however it is greatly supported to be part of a comprehensive multidisciplinary approach of non-medication treatment for chronic pain.
|
References
Yoga
Bramberg. E.B., Bergstrom, G., Jensen, I., Hagberg, J. & Kwak, L. (2107). Effects of yoga, strength training and advice on back pain: A randomized controlled trial. BMC Musculoskeletal Disorders, 18.132. DOI 10.1186/s12891-017-1497-1
Cramer, H., Lauche, R., Hohmann, C., Langhorst, J. & Dobos, G. (2013) Yoga for chronic neck pain: A 12-month follow-up. Pain Medicine, 14, 541-548.
Goncalves, A.V., Barros, N.F. & Behamondes, L, (2017). The practice of hatha yoga for the treatment of pain associated with endometriosis. The Journal of Alternative and Complementary Medicine, 23(1), 45-52. DOI: 10.1089/acm.2015.0343
Monro, R., Bhardwaj, A.K., Gupta, R.K., Telles, S., Allen, B. & Little, P. (2015). Disc extrusions and bulges in nonspecific low back pain and sciatica: Exploratory randomised controlled trial comparing yoga therapy and normal medical treatment. Journal of Back and Musculoskeletal Rehabilitation 28, 383–392. DOI 10.3233/BMR-140531
Monson, A.L., Chismark, A.M., Cooper, B.R. & Krenik-Matejced, T.M, (2017). Effects of yoga on musculoskeletal pain. The Journal of Dental Hygiene, 91(2), 15-21.
Saper, R.B., Lemaster, C.M., Elwy, A.R., Paris, R., Herman, P.H., Plumb, D.N., Sherman, K.J., Groessi, E.J., Lynch, S., Wang, S. & Weinberg, J. (2017). Yoga versus education for veterans with chronic low back pain: Study protocol for a randomized controlled trial. Trials 17, 224, DOI 10.1186/s13063-016-1321-5
Satyanand, V., Gopalakrishnaiah, T., Pannerselvam, E., Mahaboobvali, S. Bashs, S.A, & Sarala, V. (2015). Effects of yogasanas on cervical spondylosis. International Archives of Integrated Medicine, 2(7) 6-10.
Shahabi, L., Naliboff, B.D. & Shapiro, D. (2016). Self-regulation evaluation of therapeutic yoga and walking for patients with irritable bowel syndrome: a pilot study. Psychology, Health & Medicine, 21(2), 176-188. http://dx.doi.org/10.1080/13548506.2015.1051557
Sutar, R., Desai, G., Varambally, S. & Ganadhar, B.N. (2016). Yoga-based intervention in patients with somatoform disorders: An open label trial. International Review of Psychiatry, 28(3), 309-315, http://dx.doi.org/10.1080/09540261.2016.1188785
|
A Prescription for Mental Health Professionals
Helping Their Client Manage their Pain without Medications
If clients come to you saying they want help with dealing with their chronic pain what would you do:
First: It is important that you ask for a release of information so that you can read their medical records and understand better what are the sources of pain and what has been attempted previously to help relieve their pain.
Second: If the clients have been to other professionals to address their pain issues then you need releases of information so that you can get reports on their treatment and progress of these clients in working with them.
Third: Before developing a plan for your clients you must be sure to do a complete Initial Clinical Assessment (http://coping.us/cliniciantreatmenttools/clinicalassessmentplan.html) which includes exploration of ACE Factors (http://coping.us/cliniciantreatmenttools/acefactors.html) and history of any other major medical, social or interpersonal traumatic events which might account for the severity and duration of their chronic pain.
Fourth: It is important once the initial assessment is completed that you then utilize Motivational Interviewing Strategies (http://coping.us/motivationalinterviewing.html) to determine if the clients are actually ready to do the work necessary to accept their pain as a reality of life, to work seriously at following through with the steps being outlined for them to pursue to lessen the impact of pain in their lives.
Fifth: Present the following outline of procedures to take to address their chronic pain:
|
1. Self-care goals: Healthy diet, Healthy 7-8 hours of sleep each night, Use of Mindfulness Meditation to lessen daily stress (http://coping.us/mindfulnessneurobiology/stressmanagement.html ) to stay centered and focused and to be at ease and relaxed to fall asleep easily each night (http://coping.us/mindfulnessneurobiology/improveyoursleep.html).
2. Exercise or movement-based treatments (e.g. Therapeutic exercise, yoga, tai chi) At the minimum-30 minutes of aerobic exercise on a daily basis (start easy just walk) and muscle stretching daily to loosen up their tightness
3. Mind-body treatment (e.g. Mindfulness-Base Stress Reduction (MBSR) or Mindfulness-Based Cognitive Behavioral Therapy (MBCBT) in group therapy and if needed in individual sessions as well.
4. Complementary modalities (e.g. Physical therapy, osteopathic manipulative treatment, chiropractic, massage) (Lemmon & Hamptom, 2018)
|
Sixth: If the clients accept the proposed model of non-medication treatment of their chronic pain then have them take the modified EXPECT Questionnaire (Jones, et al., 2016) to determine their level of motivation and belief that the proposed intervention program will have successful outcome in helping them cope with their chronic pain.
|
EXPECT Questionnaire (modified)
I am now going to ask you a series of questions about the effects that the above treatment plan presented to you may have on your chronic pain and on how chronic pain impacts your life. In each case, the question is asking about the results at the end of the treatment period.
Chronic Pain Questions:
1.How much change do you hope for in your pain? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “complete relief.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse..........................Complete Relief
2.How much change do you realistically expect in your pain? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “complete relief.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse..........................Complete Relief
Impact of chronic pain on life questions:
3.How much change do you hope for in the impact of chronic pain on your life? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “pain no longer impacts my life.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse......................... Pain No Longer Impacts My Life
Impacts My Life
4.How much change do you realistically expect in the impact of your pain on your life? Please answer on a scale of 0 to 10, where 0 is “no change or worse”, and 10 is “pain no longer impacts my life.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse...........................Pain No Longer Impacts My Life
Sleep/Mood/Energy:
The next set of questions asks about areas of your life such as sleep, mood, and energy. If any of these questions are not relevant for you because your pain does not impact that area of your life, please answer Not Applicable.
5.How much change do you realistically expect in your pain-related sleep problems? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “back pain no longer affects my sleep.” If pain does not impact your sleep, please choose “not applicable.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse..........................Pain No Longer Affects My Sleep
6. How much change do you realistically expect in your mood or irritability? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “pain no longer affects my mood.” Or you may choose “not applicable.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse.......................... Pain No Longer Affects My Mood or Irritability
7. How much change do you realistically expect in your energy? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “pain no longer affects my energy.” Or you may choose “not applicable.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse......................... Pain No Longer Affects My Energy
Coping Question:
The next question is about your expectations about coping with your pain.
8. How much improvement in your ability to cope with pain do you realistically expect as a result of your proposed treatment plan presented to you. Please answer on a scale of 0 to 10, where 0 is “no improvement” and 10 is “extreme improvement.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Improvement.............................Extreme Improvement
Limitations due to chronic pain questions:
The following questions are about effects that your proposed treatment plan presented to you may have on your physical limitations due to your pain. In each case, the question is asking about the results at the end of the treatment period. If these questions are not relevant for you because you do not have any physical limitations due to your pain, please choose “not applicable.”
9. How much change do you hope you will have in your pain–related physical limitations? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “limitations completely resolved.” Or you may choose “not applicable.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse...........................Limitations Completely Resolved
10. How much change do you realistically expect in your pain-related physical limitations? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “limitations completely resolved.” Or you may choose “not applicable.”
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse...........................Limitations Completely Resolved
Impact of chronic pain on specific areas of life questions:
The next questions to ask about the effects that the proposed treatment plan may have on the impact of your pain on specific areas of your life. In each case, the question is asking about the results at the end of the treatment period. If any of these questions are not relevant for you because your pain does not impact that area of your life, please choose “not applicable.”
11. How much change do you realistically expect in the impact of your pain on your work, including housework? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “pain no longer impacts my work,” including housework. Or you may choose “not applicable” if your pain does not impact your work/housework now.
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse.......................... Pain No Longer Impacts my Work
12. How much change do you realistically expect in the impact of your pain on your social and recreational activities? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “pain no longer impacts my social and recreational activities.” Or you may choose “not applicable” if your pain does not impact your social and recreational activities now.
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse...........................Pain No Longer Impacts my
Social and Recreational Activities
13. How much change do you realistically expect in the impact of your pain on your daily activities? Please answer on a scale of 0 to 10, where 0 is “no change or worse” and 10 is “pain no longer impacts my daily activities.” Or you may choose “not applicable” if your pain does not impact your daily activities now.
0.....1.....2.....3.....4.....5.....6.....7.....8.....9.....10
No Change/Worse...........................Pain No Longer Impacts My Daily Activities
|
Seventh: Enroll your Chronic Pain Management clients in either MBSR or MBCBT in your office either in a group and/or individually. Keep up on the progress of your clients’ diet management, exercise schedule, sleep record and participation in any other complementary modalities. Send weekly progress reports to your clients' primary care physicians during the entire course of their treatment plan with you.
Eighth: Once the proposed length of time of treatment approaches have the clients give their evaluation of their progress and come to an agreement when their formal sessions with you in your office would end.
|
Website Resources on Pain Management
Narcan Information and video available at; narcan.com
|
Apps for Pain Management
Smiling Mind Smiling Mind is a free web and app-based program developed by psychologists and educators to help bring balance to people's lives. Just as we eat well and stay fit to keep our body healthy, mindfulness meditation is about mental health and looking after the mind. Smiling Mind is a 100% not-for-profit organization that works to make mindfulness meditation accessible to all. At https://itunes.apple.com/ca/app/smiling-mind/id560442518?mt=8
Stop, Breathe & Think Meditation for Calm & Sleep. Meditation & mindfulness to help you feel strong, connected and inspired through life’s ups and downs. Voted Best Health App, Webby People’s Voice Award. Meditate with a community! Over 3,500,000 downloads and 11 million emotional check-ins and counting! Stop, Breathe & Think, has a unique approach that allows you to check in with your emotions, and then recommends short, guided meditations, yoga and acupressure videos, tuned to how you feel. Our personalized meditation and mindfulness experience has been featured by the Today Show, Apple, GQ, Cosmopolitan and more. At https://itunes.apple.com/ca/app/stop-breathe-think/id778848692?mt=8
Headspace: Meditation - Breathe, sleep, relax & focus. Headspace is the simple way to reframe stress. Sleep trouble? Meditation creates the ideal conditions for a good night’s rest. Relax with guided meditations and mindfulness techniques that bring calm, wellness and balance to your life in just a few minutes a day. Get more from your day through mindfulness, be less distracted and reactive, and focus on the things that matter most to you. Our Basics course is completely free and will teach you the fundamental techniques of meditation and mindfulness. At https://itunes.apple.com/us/app/headspace-meditation/id493145008?mt=8
The Mindfulness Training App Start meditating right away with a wide variety of practices and styles presented by expert teachers. Though you may have heard about some of the many benefits of meditation—like better health and more peaceful relationships—perhaps you’ve not had the time or resources to learn more. If you’re ready to start a meditation practice of your own—one that is suitable for you and your unique approach to life—The Meditation Experience app was designed for you. At https://itunes.apple.com/ca/app/the-mindfulness-training-app/id687853790?mt=8
Dream Ez - Unfortunately for many people the nightmares can leave you tired during the day. And feeling sleepy all the time can make it that much harder to recover. Dream EZ is based on the principles of imagery rehearsal therapy (IRT). This therapy can help change nightmares into less disturbing dreams so you can get a better night’s sleep. Imagery Rehearsal Therapy (IRT) is an evidence-based treatment for reducing nightmares. The goal of IRT is to reduce the frequency and intensity of nightmares. By doing so, people also find that their sleep, anxiety, and depression symptoms improve.At: https://itunes.apple.com/us/app/dream-ez/id1096134340?mt=8
Migraine Buddy is an advanced migraine headache diary and tracking app designed with neurologists and data scientists. at https://itunes.apple.com/us/app/migraine-buddy/id975074413?mt=8
Cara: Food, Mood, Poop Tracker IBS, Symptom, Medication Diary Cara is the easiest way to monitor your (digestive) health. Developed by doctors, Cara helps you to understand the connection between your mind, gut, nutrition & wellbeing. Track food, stress, poop and tummy pain with a few taps. Add individual factors to create your own personalized health diary. At https://itunes.apple.com/us/app/cara-food-mood-poop-tracker/id1133687886?mt=8
Symple Symptom Tracker 4+Live your best life, every day. Symple is the easiest way to track how you feel, to monitor your health, and to improve your wellbeing. Designed by both clinicians and regular people, Symple is an enjoyable way to connect to better health. https://itunes.apple.com/us/app/symple-symptom-tracker/id479818115?mt=8
What's Up? - A Mental Health App What's Up? is a fantastic free app utilising some of the best CBT (Cognitive Behavioural Therapy) and ACT (Acceptance Commitment Therapy) methods to help you cope with Depression, Anxiety, Anger, Stress and more! With a beautiful, modern design, simple heading and easy-to-follow methods, you can get to what helps you the most in seconds! At https://itunes.apple.com/us/app/whats-up-a-mental-health-app/id968251160?mt=8
|
Stress Relaxation and Natural Pain Relief
Relaxation Techniques for Natural Pain Relief
Chronic pain is complex. Research over the past 25 years has shown that pain is influenced by emotional and social factors. These need to be addressed along with the physical causes of pain. Chronic stress is one factor that contributes to chronic pain. The good news is that you can get natural pain relief by making relaxation exercises a part of your pain-management plan.
To understand how natural pain relief works, it's important to understand how stress affects your body. Pain and stress have a similar effect on the body: your heart rate and blood pressure rise, breathing becomes fast and shallow, and your muscles tighten.
You can actually feel your body's response when you're faced with a sudden, stressful event, such as fearing that a car is about to hit you. The car misses you and, in time, your system returns to normal. You relax.
With chronic stress, such as worrying about health or finances, feeling stuck in a bad job or marriage, or fearing that something bad will happen, the nervous system keeps the body on alert. This takes a big toll on your body. Levels of stress hormones increase, and muscles remain in a nearly constant state of tension.
Chronic stress hurts.
Here's just one example: Studies that measure site-specific muscle tension in patients with chronic back pain have shown that simply thinking or talking about a stressful event dramatically increases tension in back muscles.
Relaxation Techniques for Natural Pain Relief
Relaxation exercises calm your mind, reduce stress hormones in your blood, relax your muscles, and elevate your sense of well-being. Using them regularly can lead to long-term changes in your body to counteract the harmful effects of stress.
Don't get stressed trying to pick the "right" relaxation technique for natural pain relief. Choose whatever relaxes you: music, prayer, gardening, going for a walk, talking with a friend on the phone. Here are some other techniques you might try:
- Foursquare breathing. Breathe deeply, so that your abdomen expands and contracts like a balloon with each breath. Inhale to a count of four, hold for a count of four, exhale to a count of four, then hold to a count of four. Repeat for ten cycles.
- Guided imagery. Breathe slowly and deeply. For example, imagine a tranquil scene in which you feel comfortable, safe, and relaxed. Include colors, sounds, smells, and your feelings. Do five to ten minutes each day.
- Self-talk. Change how you think about your pain and yourself. For example, change "Pain prevents me from keeping house the way I used to -- I'm a failure" to "No one will die if the house isn't perfect. I can get a lot done by breaking down tasks into baby steps."
- Hypnosis. Hypnotherapists can induce hypnosis and implant suggestions, such as, "You're going to sleep soundly tonight." Audiotape the session so that you can repeat it at home.
- Mindfulness meditation. Sit or lie quietly and notice your breathing without controlling it. If pain or thoughts interfere, simply notice them without trying to push them away. Think of them as a cloud passing over; then return to observing your breath. Do this for about 20 minutes.
Adapted from WebMD at https://www.webmd.com/pain-management/guide/stress-relief-for-pain
|
11 Tips for Living With Chronic Pain
1. Learn deep breathing or meditation to help you relax.
Deep breathing and meditation are techniques that help your body relax, which may ease pain. Tension and tightness seep from muscles as they receive a quiet message to relax. Although there are many ways to meditate, the soothing power of repetition is at the heart of some forms of meditation. Focusing on the breath, ignoring thoughts, and repeating a word or phrase -- a mantra -- causes the body to relax. While you can learn meditation on your own, it helps to take a class. Deep breathing is also a relaxation technique. Find a quiet location, a comfortable body position, and block out distracting thoughts. Then, imagine a spot just below your navel. Breathe into that spot, filling your abdomen with air. Let the air fill you from the abdomen up, then let it out, like deflating a balloon.
2. Reduce stress in your life. Stress intensifies chronic pain.
Negative feelings like depression, anxiety, stress, and anger can increase the body's sensitivity to pain. By learning to take control of stress, you may find some relief from chronic pain. Several techniques can help reduce stress and promote relaxation. Listening to soothing, calming music can lift your mood -- and make living with chronic pain more bearable. There are even specially designed relaxation tapes or CDs for this. Mental imagery relaxation (also called guided imagery) is a form of mental escape that can help you feel peaceful. It involves creating calming, peaceful images in your mind. Progressive muscle relaxation is another technique that promotes relaxation.
3. Boost chronic pain relief with the natural endorphins from exercise.
Endorphins are brain chemicals that help improve your mood while also blocking pain signals. Exercise has another pain-reducing effect -- it strengthens muscles, helping prevent re-injury and further pain. Plus, exercise can help keep your weight down, reduce heart disease risk, and control blood sugar levels -- especially important if you have diabetes. Ask your doctor for an exercise routine that is right for you. If you have certain health conditions, like diabetic neuropathy, you will need to be careful about the types of activities you engage in; your doctor can advise you on the best physical activities for you.
4. Cut back on alcohol, which can worsen sleep problems.
Pain makes sleep difficult, and alcohol can make sleep problemsworse. If you're living with chronic pain, drinking less or no alcohol can improve your quality of life.
5. Join a support group. Meet others living with chronic pain.
When you're with people who have chronic pain and understand what you're going through, you feel less alone. You also benefit from their wisdom in coping with the pain. Also, consider meeting with a mental health professional. Anyone can develop depression if he or she is living with chronic pain. Getting counseling can help you learn to cope better and help you avoid negative thoughts that make pain worse -- so you have a healthier attitude. Asking for help is a sign of strength, not weakness.
6. Don't smoke. It can worsen chronic pain.
Smoking can worsen painful circulation problems and increase risk of heart disease and cancer.
7. Track your pain level and activities every day.
To effectively treat your pain, your doctor needs to know how you've been feeling between visits. Keeping a log or journal of your daily "pain score" will help you track your pain. At the end of each day, note your pain level on the 1 to 10 pain scale. Also, note what activities you did that day. Take this log book to every doctor visit -- to give your doctor a good understanding of how you're living with chronic pain and your physical functioning level.
8. Learn biofeedback to decrease migraine and tension headache pain.
Through biofeedback, it's possible to consciously control various body functions. It may sound like science fiction, but there is good evidence that biofeedback works -- and it's not hard to master. Here's how it works: You wear sensors that let you "hear" or "see" certain bodily functions like pulse, digestion, body temperature, and muscle tension. The squiggly lines and/or beeps on the attached monitors reflect what's going on inside your body. Then you learn to control those squiggles and beeps. After a few sessions, your mind has trained your biological system to learn the skills.
9. Get a massage for chronic pain relief.
Massage can help reduce stress and relieve tension -- and is being used by people living with all sorts of chronic pain, including back and neck pain.
10. Eat a healthy diet if you're living with chronic pain.
A well-balanced diet is important in many ways -- aiding your digestive process, reducing heart disease risk, keeping weight under control, and improving blood sugar levels. To eat a low-fat, low-sodium diet, choose from these: fresh fruits and vegetables; cooked dried beans and peas; whole-grain breads and cereals; low-fat cheese, milk, and yogurt; and lean meats.
11. Find ways to distract yourself from pain so you enjoy life more.
When you focus on pain, it makes it worse rather than better. Instead, find something you like doing -- an activity that keeps you busy and thinking about things besides your pain. You might not be able to avoid pain, but you can take control of your life.
Adapted from WebMD at: https://www.webmd.com/pain-management/guide/11-tips-for-living-with-chronic-pain#1
|
Pain Management: Drug Tolerance and Addiction
Some medications used to treat pain can be addictive. Addiction is different from physical dependence or tolerance, however. In cases of physical dependence, withdrawal symptoms occur when a substance suddenly is stopped. Tolerance occurs when the initial dose of a substance loses its effectiveness over time. Addiction is a psychological and behavioral response that develops in some people with the use of narcotic pain medicines. People who take a class of drugs called opioids for a long period of time may develop tolerance and even physical dependence. This does not mean, however, that a person is addicted. In general, addiction occurs in only a small percentage of people when narcotics are used under proper medical supervision.
Addictive Pain Medications
Opioids, a family of drugs that have effects similar to those of opium or morphine, can be addictive. They include:
- Codeine
- Fentanyl (including brand name Duragesic)
- Oxycodone (including brand name OxyContin, Percocet, Percodan, Tylox, and Roxicet))
- Morphine (including brand name MS Contin)
- Meperidine (including brand name Demerol)
- Hydrocodone (including brand name Vicodin and Lortab)
- Hydromorphone (including brand name Dilaudid)
Who Is at Risk for Addiction?
Most people who take their pain medicine as directed by their doctor do not become addicted, even if they take the medicine for a long time. However, some people may be at a higher risk of becoming addicted than others. People who have been addicted to substances in the past or those with a family member who is or has been addicted to drugs or alcohol may be at increased risk of becoming addicted to narcotics.
How to Prevent Addiction
The key to avoiding addiction is to take your medicine exactly as your doctor prescribes.
Share with your doctor any personal and/or family history of substance abuse or addiction. Your doctor needs this information to prescribe the medicines that will work best for you. Fears about addiction should not prevent you from using narcotics to effectively relieve your pain. Remember, it is common for people to develop a tolerance to their pain medication and to need higher doses to achieve the same level of pain relief. Such a situation is normal and is not a sign of addiction. However, you should talk to your doctor if this effect becomes troubling.
Adapted from WebMD at: https://www.webmd.com/mental-health/addiction/drug-tolerance-addiction
|
Pain Rehabilitation
Learn about the Pain Rehabilitation Model at: https://www.ypo.education/pain-management/pain-rehabilitation-t324/video/
Chronic pain is a pain lasting beyond six months secondary to a condition affecting either a specific part of the body or the whole body. The standard modalities of treatment such as rest, medications and surgery do not provide adequate benefit for patients with chronic pain. Persistent chronic pain can result in narcotic dependence, insomnia, sexual dysfunction, physical weakness, mood disturbance, and depression. This condition is known as chronic pain syndrome.
In certain cases, chronic pain syndrome may progress to a more severe condition known as catastrophic chronic pain syndrome (CCPS).
Hyperalgesia is a condition characterized by increased sensitivity to the pain that can be secondary to chronic pain syndromes or drugs such as narcotics and benzodiazepines.
Associated conditions.
Chronic pain syndrome may be associated with various disease conditions including:
- Low back pain.
- Neck pain.
- Arthritis.
- Headaches.
- Fibromyalgia.
- Complex regional pain syndrome (CRPS).
- Nerve damage.
- Trauma.
- Multiple sclerosis.
- Gastrointestinal illness.
- Joint degeneration.
- Reflex sympathetic dystrophy (RSD).
- Other chronic medical conditions.
Treatment.
The objective of treatment is to reduce or eliminate the pain; by concentrating on the psychological and physical factors affecting the individual, through a multidisciplinary team approach. The basic steps in the treatment of chronic pain syndrome and CCPS include:
- Adopt a biopsychosocial model of patient care: After chronic pain syndrome or CCPS is diagnosed, a special pain management team is organized comprised of doctors and therapists with good communication skills to ensure a rapid and precise treatment. The team is usually specialized in gym and aquatic exercise, stress management, diet, substance dependence, medical detoxification, cognitive therapy, psychotherapy, massage, family therapy and other relevant specialties. This approach is also known as pain rehabilitation.
- Prevent worsening of the condition: In cases of CCPS standard pharmacologic agents are not very effective. Long-term use of narcotic therapy can cause opioid-induced hyperalgesia, addiction, constipation, sleep disorders, and a decrease in testosterone levels. Therefore, in these patients opioid and benzodiazepine detoxification may be recommended. In contrast to normal pain treatment, excessive rest can result in muscular atrophy and weight gain in patients with CCPS. Therefore, physical therapy or regular exercise is recommended in these patients.
- Medical and psychological history of the patient: Prior to initiation of treatment, a complete medical history of the patient including history of childhood abuse, addiction, previous injuries, and details of any previous therapies with medical records should be obtained. Along with this a psychological history including family expectations, work expectations, and any other data essential for psychotherapy should be obtained.
- Treat the syndrome: In pain rehabilitation, the underlying condition is treated rather than treating only the pain. Improvement in symptoms helps the patient to learn self-management of daily activities, stress, catastrophic thinking and also helps in opioid detoxification. Pain syndromes involve various factors that induce hyperalgesia that include excessive use of opioids, depression, cognitive distortions and inactivity. Therefore, narcotic detoxification, cognitive-behavioral therapy and exercise are an integral part of CCPS treatment.
Pain rehabilitation.
Pain rehabilitation includes various interventions such as muscle reactivation, physical therapy, biofeedback training, education classes, psychotherapy, nutritional instruction, family counseling, chemical detoxification and medical management intended to reduce pain and improve function in individuals suffering from chronic pain and other related conditions. Pain rehabilitation programs may last from 6 days to 6 weeks or longer, depending upon the condition of the patient.
Types of pain rehabilitation.
Based on the severity of the condition, involvement of the medical staff, and the condition of the patient, pain rehabilitation programs can be categorized into three types:
Primary or acute care.
Secondary rehabilitation.
Tertiary rehabilitation.
- Primary care includes simple non-surgical interventions for the management of symptoms causing pain. This program may last for 6-8 weeks.
- Secondary rehabilitation is given to patients not responding to primary care; it requires a large team of doctors and therapists from different specialties and the treatment lasts for 4-6 months.
- Tertiary rehabilitation is given to patients with critical conditions; it employs advance facilities and focuses on the different aspects and requirements of the individual patient.
Pain rehabilitation is used for the management of patients suffering from chronic pain conditions. It is coordinated by a multidisciplinary team, with the objective to restore the physical and mental health of the patient and also to help the patients perform their daily routine activities without any pain or discomfort.
|
Back and Neck Exercises
View Back and Neck Exercises at: https://www.ypo.education/pain-management/back-and-neck-exercises-t332/video/
Strengthening exercises are specifically designed physical activities that improve muscle strength and flexibility. Strengthening exercises help an individual lose body fat, gain muscle mass, muscular endurance and ensure a healthy body.
Back strengthening exercises.
Back strengthening exercises are designed to improve strength, endurance and flexibility of the back muscles. These include specific exercises for the back and abdomen. Forward and backward activities of the spine require strong back and abdomen muscles to counter balance the movement of the spine.
Back exercises.
- Position: Lying on the back Lie on the back and keep the knees flexed. Keep the feet and palms flat on the floor. Tighten the abdominal muscle to maintain neutral position of the spine. This is the starting position for back exercises.
- Bridge-up. Lie on the back with knees bent. Keep the feet flat on the floor and arms at the sides. Now, gradually raise the hips little by little. Remember to raise the hips without arching the back. Tighten the stomach to avoid pushing out of the stomach which may tend to arch the back. Hold the position for 5 seconds. Afterwards, slowly come back to the starting position. Repeat the technique five times. The Bridge-up exercise helps to strengthen buttock muscles.
- Partial curl-up Lie on the back with flexed knees. Keep the feet flat on the floor and arms at the sides. Cross the arms loosely over the chest. Tighten the abdomen and curl halfway up. Keep the middle and lower back flat on the floor and raise the head and shoulders from the floor. Hold the position for a few seconds and then return to the relaxed position. Repeat the technique for five times. The partial curl-up exercise strengthens the abdominal muscles.
- Trunk rotation. Lie on the back and keep the knees bent. Keep both feet and shoulders flat on the floor. Gradually drop the knees to one side and turn the head in the opposite direction. Hold the position for 20 seconds and gradually come to the previous position. Repeat the technique three times. The trunk rotation exercise strengthens the lower back muscles.
Position: Lying on the stomach
- Press-up Lie on the floor facing down. Keep the feet slightly apart and forehead on the floor with arms bent at the elbow above the head. Push the body up on the forearms while keeping the neck straight. Lift the abdomen away from the floor. Hold for 20 seconds and slowly come back to the relaxed position. Repeat the exercise 3 to 5 times. The press up exercise strengthens the lower back muscles.
- Opposite arm and leg raise. Lie face down, forehead on the floor and keep the arms above the head without flexing the elbows and wrists. Slowly lift the arm and the opposite leg, and tighten the lower back and buttock muscles. Hold for 2 seconds and come back to the starting position. The technique is practiced with the other arm and its opposite leg as well. Repeat the procedure with each arm for 3 to 5 times. This exercise targets your core and lower back.
- Superman or swimming. Lie on the stomach, forehead on the floor and keep the arms above the head without bending the elbows and wrists. Gradually lift both arms and legs from the ground. Tighten the lower back and muscles of the buttocks. Hold the position for 2 seconds and come back to the starting position. Repeat the exercise for 10 times. This exercise also targets your lower back.
Position: On hands and knees.
- Cat stretch. Keep the body in a crawling position. Evenly distribute the body weight on the hands and knees. Gradually tighten the abdominal and buttock muscles, and press the back upward. Let the head drop forward. Hold the position for five seconds. Now slowly relax the abdominal and buttock muscles, lift the head and bring back the spine to normal position. Once again tighten the muscles of the abdomen and buttock and press the back downwards. Move the head forward and upward. Hold the position for five seconds. Now slowly relax and come back to the normal position. Repeat the process 10 times. The Cat stretch exercise strengthens core and lower back muscles.
- Arm reach. Keep the body in crawling position and distribute the body weight evenly over the hands and knees. Raise one arm straight out in front. Do not raise head and do not allow the supporting shoulder to drop. Tighten the abdominal muscles to prevent sagging of the trunk. Hold the position for five seconds and lower the arm. Repeat the process 10 times and alternate using the opposite arm. This is a core strengthening exercise.
- Arm reach with leg reach. With the body in crawling position, raise one leg straight back and extend the opposite arm straight forward. Avoid arching the back, or sagging the head or body. Tighten the abdominal muscles and hold for five seconds. Repeat the process 10 times and alternate using the other leg and its opposite arm. This exercise targets the core and low back.
- Neck strengthening exercises. Neck strengthening exercises are a group of exercises that are designed to improve muscle strength, endurance, and flexibility of the neck muscles. These exercises improve posture, relieve chronic or recurrent neck pain and radiating pain from the upper back and help prevent problems related to spinal discs.
- Chin tuck. In a comfortable sitting or standing position, keep the back and neck straight and shoulders slightly back. Slowly tuck the chin until a gentle stretch is felt over the cervical (neck) area. Keep the eyes and nose facing forward. Hold the position for 3 seconds. Repeat 10 times.
- Neck press In a comfortable sitting or standing position, keep the back and neck straight. Similarly, keep the eyes and nose straight in the forward position. Place the palm of the hand onto the forehead and press the palm against the forehead. Now push the forehead against the palm with the help of neck muscles. Hold the position for three seconds and repeat the technique for 10 times. Cup both palms and place at the back of the head. Now try to push the head forward with the palms and resist the movement by pressing the head back towards the palm with the help of neck muscles. Hold for three seconds and repeat for ten times. Place the hand at the side of the head. Slowly push the head with the palm while resisting the force by the head with the neck muscles. Hold the position for three seconds and repeat for ten times.
- Shoulder blade squeeze This exercise can be initiated either in a sitting or standing position. Keep the chin slightly tucked in, bend the shoulders slightly back and elbows forward. Gradually squeeze the shoulder blades together and raise the elbows or lower arms up. Press the shoulder blades down towards the mid back. Hold the position for three seconds and repeat for ten times.
Muscles of the back and neck have many complex functions that control posture and movements of the back and neck. Strengthening exercises of these areas improve the strength, flexibility and endurance of the muscles and help to maintain general fitness of the body and prevent further problems related to the back and neck.
|
Neck Pain
View the video on neck pain at: https://www.ypo.education/pain-management/neck-pain-t481/video/
Neck pain is a common condition that affects most people at some point in their lives. The causes can be varied and can affect different structures in the neck. Neck pain can result from muscle strain due to poor posture and long work hours, osteoarthritis, which is wear and tear of the cartilage or discs in the joints, bony overgrowths or spurs, compression of spinal nerves, also called pinched nerves, neck fractures, slipped discs, whiplash, a forceful jerking of the neck causing soft tissue injury, and also from diseases such as meningitis, rheumatoid arthritis and cancer.
|
Peripheral Neuropathy
See the video on peripheral neuropathy at: https://www.ypo.education/pain-management/peripheral-neuropathy-t335/video/
The nervous system consists of the central nervous system (CNS) and the peripheral nervous system (PNS). The CNS is comprised of the brain and spinal cord, while the PNS comprises of nerves that carry information to and from the brain to the rest of the body. There are three types of nerves that are included in the PNS:
- Autonomic nerves that control BP, bladder functions and sweat levels;
- motor nerves that control the muscles, and
- sensory nerves that transfer sensations like cold, heat or pain to the brain.
Peripheral neuropathy is a condition characterized by damaged nerves that cause pain. When this condition affects one nerve, it is called mononeuropathy; when several nerves are affected, it is polyneuropathy; and when 2 or more nerves are involved in different areas, it is termed as multiple mononeuropathy. Peripheral neuropathy is a comparatively common disease that usually affects older people.
Causes.
Diabetes is the most common cause of peripheral neuropathy. At least half of all diabetics develop some form of neuropathy during the course of the disease.
Other factors that can cause peripheral neuropathy are:
- Excessive alcohol intake, which leads to poor dietary choices.
- Autoimmune diseases like lupus and rheumatoid arthritis.
- Exposure to toxic substances like heavy metals and certain medications, like chemotherapy.
- Viral or bacterial infections.
- Trauma or compression of the nerves.
- Tumor on or surrounding the nerves.
- Vitamin deficiencies.
Signs and Symptoms.
Symptoms depend on the type of the affected nerve. Common signs and symptoms include:
- Numbness and tingling sensation in the feet or hands that can slowly spread to the legs and arms.
- Burning or sharp electric pain.
- Sensitivity to touch or heat.
- Impaired coordination.
- Muscle weakness or paralysis.
- Bowel or bladder incontinence.
- Foot infection and ulcers.
Diagnosis.
Peripheral neuropathy involves the exact detection of nerve damage and its cause, which is difficult to diagnose. Your doctor will review your medical history and family history for neurological diseases and will conduct physical and neurological examinations for muscle strength, sensation, posture and coordination.
Your doctor may order other tests including:
- Blood tests for vitamin, sugar and thyroid levels and liver and kidney function.
- Computed tomography (CT) scan or MRI to detect herniated disks or spinal tumors.
- Nerve function tests using electromyography to measure the electrical activity of the nerves.
- Nerve biopsy, in which a part of the damaged nerve is removed to test for abnormalities.
- Lumbar puncture to test cerebrospinal fluid in the lower back for signs of disease.
Treatment.
The main aim of treatment is to control the underlying cause of peripheral neuropathy and manage pain. Symptoms of peripheral neuropathy can be relieved with:
Medications.
- Your doctor may prescribe pain killers, anti-seizure and antidepressant drugs, and topical medications.
- Neuromodulation such as Spinal cord stimulation or peripheral field stimulation- Your doctor will pass a gentle electric current through two electrodes placed on the painful areas of your body. Your pain will reduce when the electric impulses travel along the nerves of the painful area, due to the stimulation of the affected nerves and production of endorphins (natural pain killers), which block the pain signals in the brain.
- Acupuncture. Your therapist will insert thin needles into the body close to the nerves. This will stimulate the nerves and release endorphins.
- Plasma exchange and intravenous immune globulin may be performed to suppress the activity of the immune system.
Prevention.
Peripheral neuropathy can be prevented by:
- Managing the underlying disease condition such as diabetes.
- Maintaining a healthy diet and lifestyle to keep your nerves healthy.
- Eating a vitamin B-12 rich diet or including supplements.
- Preventing nerve damage by avoiding repetitive motions, restricted positions, toxic chemicals, and excessive alcohol.
Peripheral neuropathy affects the peripheral nerves causing severe pain. Symptoms can be relieved with medications and various therapies that block the pain causing nerve signals to the brain. A healthy lifestyle and management of diabetes will help prevent peripheral neuropathy.
|
Fibromyalgia
Fibromyalgia video available at: https://www.ypo.education/pain-management/fibromyalgia-t346/video/
Fibromyalgia is a complex chronic disorder characterized by widespread body pain that affects individuals physiologically, mentally and socially. Fibromyalgia is associated with pain over multiple tender points on the body including tenderness of the joints, muscles, tendons and other soft tissues. In addition, the patient may experience fatigue, sleep disturbances, depression, and anxiety. In severe cases, the condition can be extremely debilitating and may interfere with daily living activities.
Causes.
The cause of fibromyalgia is not known, but certain factors such as sleep disorders, physical or emotional trauma, viral infections, and abnormal pain perception can trigger fibromyalgia. Middle aged women are at an increased risk of developing the condition. Several other conditions such as chronic neck or back pain, chronic fatigue syndrome, Lyme disease, hypothyroidism, sleep and depressive disorders may mimic the symptoms of fibromyalgia and may coexist with it.
Symptoms.
The predominant symptom of fibromyalgia is generalized body pain. The intensity of pain varies from mild to severe. Tender points, localized painful areas in the neck, shoulders, back, hips, arms or legs, are present. Any touch or firm pressure over the tender points may induce the pain sensation. The pain may either be continuous or there may be a diurnal variation in pain, with an aggravation of the pain during the night. The pain may either be aching in nature or a shooting, burning pain that may increase with stress, anxiety, physical activity and cold or damp weather. Most people with fibromyalgia also experience fatigue, depression, and sleep disorders where they wake up with a feeling of tiredness despite long periods of sleep. People with fibromyalgia may also have other associated symptoms such as irritable bowel syndrome (IBS), headache, memory and concentration disorder, numbness and tingling sensation in the hands and feet, irregular heartbeat, and decreased ability to exercise.
Diagnosis.
The diagnostic criteria for fibromyalgia includes:
- Widespread pain lasting for at least three months.
- Pain in at least 11 of the 18 tender points including elbows, buttocks, chest, knees, shoulders, lower back, neck, rib cage, and thighs.
- Blood and urine tests may be recommended to rule out other conditions with similar symptoms.
Treatment.
The treatment for fibromyalgia is aimed at resolution of the symptoms and helping the patient to cope with the symptoms and improve their quality of life. Treatment options for fibromyalgia include physical therapy, fitness and exercise program, and stress relief techniques such as light massage or other relaxation techniques. Swimming or exercising in a warm or heated pool may be beneficial to reduce pain, joint stiffness and relax the joints. If required medication may be prescribed to improve pain tolerance and avoid sleep disturbances. Several medications such as antidepressants, muscle relaxants, anticonvulsants (anti-seizure), and pain killers can be prescribed for initial pain management. These medications provide symptomatic relief from pain and also improve quality of sleep.
Cognitive behavioral therapy (CBT) is an important aspect of fibromyalgia treatment and helps in modification of an individual’s response to pain. Support groups may be also helpful in managing fibromyalgia. Psychotherapy or counselling also may be useful to deal with issues related to fibromyalgia. A well-balanced diet, exercise program, abstinence from caffeine, following a regular sleep pattern, performing some relaxation techniques and being educated about the condition are all helpful to live a healthy life with fibromyalgia. Other therapies such as acupuncture therapy also may be applicable to relieve the symptoms.
In severe cases the patient may require a referral to a pain clinic. Fibromyalgia is a chronic disorder characterized by widespread pain and tenderness over the tender points of various parts of the body
|
Headache
See the video on Headache at: https://www.ypo.education/pain-management/headache-t328/video/
A headache is pain or discomfort anywhere in the region of the head or neck. Headaches are the most common health complaints experienced by every person at some point during their life. Most headaches are not serious and can be treated with medications and lifestyle changes. There are many different types of headaches and it is important to know the particular type of headache you have and also methods to treat the same.
Types.
Depending upon the cause, headaches can be divided into three major categories:
Primary headaches: Primary headaches are those headaches that are not associated with other medical conditions. The most common types of primary headaches include:
- Tension headaches: Tension headaches are the most common type of headaches that occur when the head and neck muscles contract. Tension headaches may occur at any age, but are most common in adults and adolescents. The muscle contractions may be caused by stress, poor posture, fatigue, eye strain, alcohol and tobacco use, and even hormonal changes in women before and after a menstrual period.
- Migraine Headache: A migraine is a common type of headache usually felt as a throbbing pain on one side of the head. The exact cause of migraine is unknown, but may occur from a series of changes in brain activity. Migraines occur more often in women than men and may run in families. Migraine attacks may be associated with alcohol use, smoking, lack of sleep, prolonged muscle tension and stress, changes in hormone levels during a woman's menstrual periods or with the use of oral contraceptives and certain foods especially chocolate, cheese, nuts, alcohol, and foods containing preservatives and artificial sweeteners.
- Cluster headaches: Cluster headache is a less common type of primary headache. Cluster headaches can occur at any age but are most common in men in their late 20s. The cause of cluster headaches is unknown, but abnormalities in an area of the brain called the hypothalamus may be involved. They also tend to run in families. Cluster headaches are triggered by certain factors such as changes in sleep patterns and use of medications such as nitroglycerin, a drug used to treat heart disease.
Secondary headaches: Secondary headaches are those that are caused by other underlying diseases. Some medical conditions that can cause secondary headaches include bleeding in the brain, brain tumors, meningitis and encephalitis.
- Cranial neuralgias, facial pain, and other headaches: Cranial neuralgia (pain coming from a nerve) is pain or discomfort in the head or neck caused by inflammation of the nerves located in the head and upper neck. Facial pain can be caused from a nerve disorder, an injury, or an infection in a structure of the face or it may occur for no known reason.
Symptoms.
People with tension headaches have generalized pain in the head and neck described as a band-like tightness or pressure.
Migraine headaches often cause a throbbing or pulsating sensation usually on one side of the head. Pain often starts as a dull ache and can worsen within minutes or hours. This type of headache may occur with symptoms such as nausea, vomiting, visual disturbances, and sensitivity to light and sound. The pain can last a few hours or even up to one or two days. Some people with migraines experience prodromal symptoms, including repeated yawning, food cravings, mood changes, and altered perception of heat and cold. These symptoms occur several hours before the headache begins.
Cluster headaches have a characteristic grouping or clustering of attacks. People with cluster headaches usually get pain once or twice daily which may last for weeks or months. This is followed by a pain free period lasting for months or years, before the headache attacks start again. Each cluster headache lasts from 30 to 90 minutes. Attacks tend to occur at the same time each day and often wake the person from sleep. The pain is extremely painful and may occur behind and around one eye. Other symptoms include stuffy nose, excessive tearing, redness in the eye, and restlessness. For some people the pain feels like a hot poker being stuck right in the eye. People with cluster headache often pace the floor, bang their heads against a wall, and can be driven to take desperate measures to relieve the pain.
Diagnosis.
Your doctor can diagnose headache by asking questions about your symptoms, family history, medical history, diet, and lifestyle. Diagnosis depends on your description about the headache, its location, length, duration, causative factors and associated symptoms. Your doctor may order the following diagnostic procedures:
- An MRI or CT scan of the head may be needed to rule out other causes of the headaches.
- An X-ray of the sinuses may be taken to evaluate sinus problems.
- Lumbar puncture: A spinal tap, also called lumbar puncture, is removal of cerebrospinal fluid, or CSF (fluid surrounding the spinal cord and the brain) from the spinal canal to diagnose disorders affecting the brain and spinal cord. This procedure may be performed to look for signs of infection and to check for bleeding around the brain.
- Temporal artery biopsy: A sample of blood vessel is taken from your temple and studied to check for signs of inflammation.
Treatment.
Your doctor may suggest keeping a headache diary to help identify your headache type and recommend effective treatment. Your headache diary should include information about the location of pain, duration, intensity, foods eaten, medications, weather conditions, daily activities, and associated symptoms.
To control tension type headaches over the counter (OTC) pain medications are prescribed.
The treatment of cluster headaches is very difficult. You may need treatment to relieve and to prevent cluster headaches. Your doctor may treat cluster headache with oxygen inhalation, a tryptan injection, and the use of intranasal applications of a local anaesthetic agent. Medications used to prevent additional headaches include blood pressure medications, antidepressant medications, and drugs used to treat seizures.
Medications for migraine headache fall into two categories:
- Abortive: These types of medications are taken during migraine attacks and are designed to stop it once it starts. Abortive medications can be taken by mouth or nasal spray or administered by self-injection. These medications work quickly and are effective in people who have nausea and vomiting with their migraine. The most commonly used abortive medications for migraine are triptants.
- Preventive: These types of medications are taken on a daily basis, to reduce the severity or frequency of the migraine attacks. Preventive medications include antidepressants, antiseizure medications, and medications used to treat high blood pressure.
You can also help reduce the frequency and severity of the attacks by stopping smoking, avoiding alcohol and any foods associated with bringing on headache.
Everyone gets an occasional headache and they are usually harmless. You should be concerned if you have headaches almost every day and if pain limits your ability to get on with life’s activities. Some headaches may be a sign of a more severe illness and therefore one should get medical attention immediately.
|
|
|