FOCUS on Intimate Partner Violence
|
|
Intimate Partner Violence -
A Training Resource
By: James J Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
Monica's Story
Monica’s childhood was destroyed by her father’s constant violence and abuse. He verbally humiliated and beat her mother and hit her and her siblings. Her mother tried to numb the abuse by drinking. At high school Monica discovered alcohol and started drinking daily to cope. Her teachers found her behavior increasingly difficult and suspended her multiple times. Monica started running away from home and living on the streets. Adult men who were grooming her for ‘prostitution’ raped her. Eventually, Monica was taken into state care. At 17, she was discharged from state care. Estranged from her parents, positive social supports, and vulnerable, she met Jim at a hotel bar. Jim was a patched gang member. He made Monica his partner. The only thing Jim had learned from his stepfather was violence. For Monica the next ten years involved: being put down in front of friends, family, and neighbors; ‘getting beaten’ – if she fought back she got it even worse; rapes; miscarriages; and, feeling guilty and disgusted with herself for using alcohol and drugs and not ‘being there’ for her children. Sarah was seen at the emergency department concussed with most of her teeth knocked out. There were more than 15 Police reports; she had taken out a protection order which Jim repeatedly breached. Her children were removed from her care and placed with relatives and this made her drink even more. Finally, Jim moved on from her and started living with another (younger) woman. Monica went to rehab and cleaned up. She got her children back from Child, Youth, and Family. A Non-Profit Housing Agency gave her a home - in a rough part of town with few community services. She had little money to do anything or go anywhere. She had debts she was paying back from her benefit, due to damage caused by Jim to previous Housing properties. All her siblings drank, and some were now gang affiliated. If they came over, they bought alcohol with them, which made it hard for her to stick to her sobriety. However, not seeing them made her feel isolated, lonely, and depressed. Monica felt judged. She heard the hurtful remarks people and professionals made about her family. She preferred the company of her siblings because at least they understood what she had been through. She met her next partner, Harry, through one of her siblings. She was wary because he was a gang member, but he seemed okay and initially he treated her much better than Jim had. Her sister said that ‘beside the hidings and all that’ Harry came across like he really cared for her. After they started living together Harry’s controlling behaviors intensified. He constantly accused her of infidelity. She was not allowed in the company of other men without him. When he was not around, he had his friends watch her. Her children were terrified of Harry and she was terrified of losing them again to Child Protective Services. Her previous experiences meant that she knew if she could not protect them from him, she could lose them to state care. She was very worried about what might happen to them in state care because her sibling’s child was sexually abused in state care. Monica was also scared to call the Police. Harry had threatened to hurt her children if she called. He had strangled her, and she knew he was capable of killing her and harming her children. In the past, whenever Jim had been arrested, he would afterwards return to her house and beat her up for having called the Police. Would Harry be locked up or would he be bailed to her address? How could the Police or the courts keep her and her children safe? She wished the neighbors would call the Police but they never did. Harry’s abuse made her feel suicidal and brought back Jim’s abuse all over again. She desperately wanted a different life for her children. One night she was so terrified of Harry, she called the Police. They arrived but she was too intimidated by Harry to make a statement. She said it was ‘just a verbal argument’. The Police issued Harry with a Police Safety Order. His reprisal was a serious beating. Refuge was not an option as she was drinking again to try to block out the abuse. She had no car and nowhere to go. Harry knew where all her siblings lived – she couldn’t go there. Eventually, she thought, he would kill her. He did.
|
|
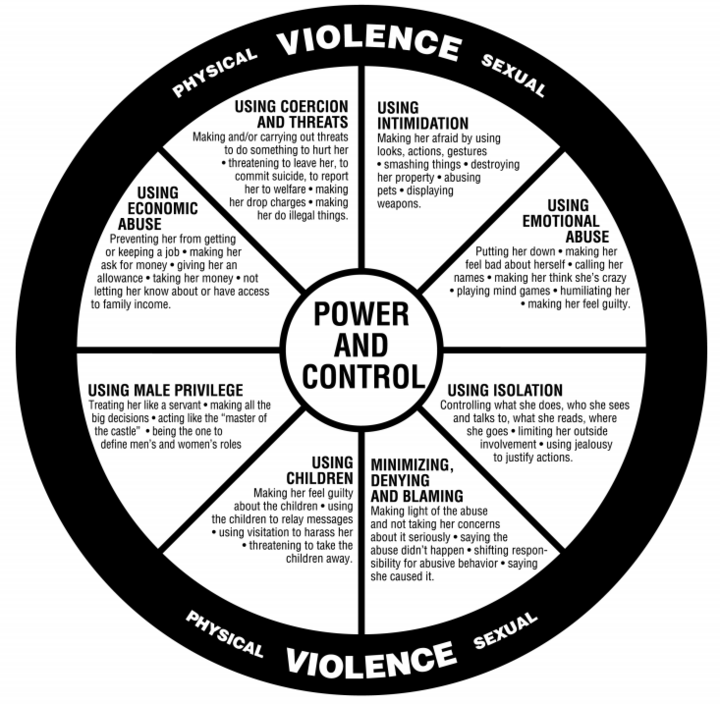
Power and Control Wheel of Factors Contributing to Intimate Partner Violence
|
Domestic violence is a pattern of behaviors used to gain or maintain power and control. The National Domestic Violence Hotline uses as its frame of reference for describing abuse the Power and Control Wheel developed by the Domestic Abuse Intervention Project in Duluth, MN. In the diagram above, the Power and Control Wheel assumes she/her pronouns for the victim and he/him pronouns for the perpetrator, but the abusive behavior that it details can happen to people of any gender or sexuality. The wheel serves as a diagram of tactics that an abusive partner uses to keep their victims in a relationship. The inside of the wheel is made up of subtle, continual behaviors over time, while the outer ring represents physical and sexual violence. Abusive actions like those depicted in the outer ring often reinforce the regular use of other, more subtle methods found in the inner ring.
The Elements of the Power and Control Wheel are:
Physical and Sexual Violence (outer ring)
Using Intimidation
Using Emotional Abuse
Using Isolation
Minimizing, Denying and Blaming
Using Children
Using Male Privilege
Using Economic Abuse
The NDV Hotline also has two additional renditions of the Power and Control Wheel which you can download by just clicking on the title:
1. The Original Power & Control Wheel
2. The Power & Control Wheel for LGBT People
Reference for Power and Control Wheel:
|
Assessment for Intimate Partner Violence During COVID-19
The COVID-19 pandemic has escalated the risks and dangers for victims of Intimate Partner Violence (IPV). Healthcare providers do not consistently screen for IPV due to limited time and resources, reluctance to possibly offend the patient, insufficient training and reimbursement, and perceived lack of institutional support (Tower, 2006). The most frequently reported barriers included personal discomfort with the issue, lack of knowledge, and time constraints (Sprague et al., 2012). Provider-related barriers were reported more often than patient-related barriers. This leads to missed opportunities for victims to access information, resources, and support. The COVID-19 pandemic has escalated the risks and vulnerabilities of victims of IPV, thus it is increasingly essential that healthcare professionals address safety and violence at home.
The risks and vulnerabilities of victims of IPV during COVID-19 are multiplied for undocumented immigrants. Undocumented immigrant women are profoundly vulnerable to IPV due to physical and social isolation, fear of law enforcement, lack of information on available resources, language barriers, and legal status. Many undocumented immigrants do not discuss IPV with healthcare providers because they cannot be sure what the providers’ responses will be, and they fear deportation and separation from their children. Anti-immigrant rhetoric from political leaders and the media has deepened this fear in recent years, leaving many victims feeling profoundly isolated from resources and support (Zero and Geary, 2020).
A study was done to develop the Healthy Relationship Assessment Tool (HEART) that assessed negative aspects of male partner involvement in women’s HIV prevention. Five constructs with theoretical relevance and good-to-strong reliability were identified: Traditional Values; Partner Support; Partner Abuse & Control; Partner Resistance to HIV Prevention; and HIV Prevention Readiness. Predicted associations between HEART constructs, and correspondence between participants’ qualitative data and HEART scores were generally correct (Tolley et al., 2020).
|
Jenny's Story
“When I met Ted everything seemed perfect. I got pregnant soon after and was so excited to be expecting our first child, I thought he would be too. When I told Ted the happy news, everything changed. He held me down and shouted at me and when I struggled to get loose, he hit me. Not long after, Ted locked me in our shed for one whole night without any food. One day he returned home from work and told me that if I didn’t terminate the pregnancy, he would kill me and the child. I decided to run to my friend’s house. But Ted found my packed suitcase and pushed me down the stairs – injuring me badly and worst of all, losing my baby. When I was in hospital, I decided to tell my story to the nurse. I felt powerless, lost and scared but the nurse helped me plan to leave. She got me details for a domestic abuse charity and, with their help, a refuge space. I was able to access a lawyer via legal aid and get a restraining order. Ted can no longer come near me.”
|
|
Pregnancy Related IPV
A significant number of pregnant women reported IPV. This emphasizes the importance of screening for IPV in these women. It is observed that women with IPV had higher psychiatric comorbidity and may require psychotherapeutic intervention (Lynegar, et al., 2020).
IPV, specifically physical and sexual violence, are associated with pregnancy complications. The results show that 31.6% of the women had experienced some form of IPV. The factors associated with IPV included husband’s alcohol habit, women who had witnessed parental violence, and women whose husbands had shown high marital controlling behavior. The high level of pregnancy complications was reported by women who had experienced sexual violence, emotional violence, and women whose husbands display three or more specific behaviors (Avanigadda & Kulasekaran, 2021).
Emotional and physical IPV and financial adversity independently and jointly increase the risk of incident homelessness among pregnant and post-partum women. The effects of emotional and physical IPV are comparable to or greater than the risk of financial adversity. Homelessness prevention policies should consider IPV victims as high-risk, regardless of financial status. Furthermore, self-reported physical IPV declines temporarily during pregnancy and up to 8 months post-partum. Screening for IPV in this period may miss high-risk individuals (Chan, et al., 2021)
|
Alexandria's Story
Alexandria an 18-year-old woman presented to her family physician for an initial obstetric examination, accompanied by her 27-year-old boyfriend. Initial history revealed that she was a gravida 1, para 0, at 16 weeks of gestation and living in a mobile home with her partner. She was strongly considering giving up the baby for adoption because of “financial and other” reasons. Answers to screening violence history questions indicated that she had been beaten by her father from preschool age until she was 13 years of age; her parents then divorced. The patient stated that her present partner had “slapped her around” on several occasions and that once she was “accidentally dragged by his truck” during an argument. He had slammed the driver's door, started the truck and put it in gear, reportedly without realizing that her dress was caught in the car door. On further questioning the patient stated that she was not happy in this relationship and in fact did not feel safe. However, she stated that she “had no place else to go” and expressed optimism about the future because her partner had begun to attend church and stated that he wanted to be a good father.
|
|
Guns Influence on IPV
Almost one-half of U.S. women will experience intimate partner violence (IPV), defined as physical, sexual, or psychological harm by a current or former partner. IPV is associated with an increased risk of homicide, with firearms as the most commonly used weapon. Ease of firearm acquisition: Women who were older (mean 44.92 years), compared to women who were younger (40 years) were more likely to describe it as easy or very easy to acquire a gun. Perceived safety in the proximity of a gun: Women with the highest ACE score were less likely to feel safe with a gun nearby. Odds of guns in the home: Women who were divorced or separated, women were widowed or single, and women who were partnered had lower odds of having a gun in the home, compared to married women. There was no significant effect of the trauma variables on the odds of having a gun at home. Conclusions: Women with more severe childhood trauma felt less safe around firearms, but trauma exposures did not predict the perception of gun prevalence in the local community or gun ownership. Instead, demographic factors of marriage predicted presence of a gun in the home (Leuenberger et al., 2021).
|
IPV affects Quality of Life of Victim and Family
An intimate relationship is an interpersonal relationship that involves physical or emotional intimacy. Those who are in such a relationship may experience violence from partners which may affect their day-to-day quality of life and thus cause a burden on the family. In a study of IPV victims The majority belonged to rural background and lower socioeconomic status. The study subjects reported poor and very poor scores in their overall quality of life and very dissatisfied and dissatisfied in their health domain. IPV also correlated with reduced quality of life, which was statistically significant. People that experience IPV have an overall reduced quality of life. Routine clinical assessment needs to be done to provide early interventions (Gopal et al., 2021).
|
Military Families and IVP
Practitioners must also consider subcultural considerations with populations such as
military families. With military deployments at the highest rate in the past seven
decades and almost 2 million children with a military parent, human service and mental healthcare professionals must be aware of the significant rates of IPV within military
families. Research suggests that IPV perpetration among veterans is almost three
times greater than civilian rates, and the violence within military families is often
more frequent and severe than in civilian families (Klostermann et al., 2012;
Tasso et al., 2016).
Some posit that these differences may be due to “cultural spillover theory”, the idea that
the use of violence in one area of life (e.g., military experience) may spill over to other
areas of life where violence is considered unacceptable (e.g., intimate relationships; Klostermann et al., 2012). Additionally, postcombat conditions and related disorders such
as traumatic brain injuries and posttraumatic stress disorder are commonly accompanied
by violent behaviors (Taft et al., 2013). Assessment of a military family’s IPV history and
types of IPV is an essential aspect of intervention. For many military families, the often
long and repeated deployments interrupt family stability and increase the risks (Rubin,
Weiss, & Coll, 2012). Practitioners should be aware of the IPV risk factors for military
families, and they should strive to be military-informed when working with military families.
They should be aware also of the potential cultural barriers to treatment, including stigmatization of mental health services, military versus civilian culture, and
warrior culture.
|
|
Jennifer' Story
I experienced years of sexual abuse during my long-term relationship with my ex-partner. After I gave birth, I told him I didn’t feel comfortable having sex as I was in a lot of pain. But he forced me to sleep with him on a daily basis when he arrived home from work, drunk and demanding. I had no money as my ex-partner controlled all the finances. He told me if I wanted to buy basic essentials, I would have to have sex in return. I began to feel worthless. To make matters worse he attended all my medical appointments so that I would not have a chance to disclose anything. The only time I spent out of the house was a short walk to take my children to school. At family gatherings, he acted the part of a devoted husband and father. I eventually fled with the help of the police and a domestic abuse charity. I spent 3 months in a refuge before moving to a rented house. The police prosecuted, my ex pleaded guilty to rape and was sent to prison. I was not aware that domestic abuse included sexual abuse. I am now a licensed practicing dentist and I volunteer to support other survivors who have been affected by domestic abuse.
|
|
Economic Factors in IPV
The prevalence of help seeking behavior among married women who experienced IPV was found to be significant. Only half of them sought help from a formal source (such as police, lawyer or doctor). Physical violence, educational attainment, a partner’s alcohol consumption, partner’s controlling behavior, partner’s employment status and wealth index were significantly associated factors with help seeking behavior among married women who experienced IPV (Mulunech et al., 2021).
|
Impact of Alcohol consumption of pepetrator in IPV
Alcohol consumption by the husband, initial place of residence, and controlling behavior by the husband were significantly associated with physical violence. Higher education status of the women, justification of violence by the women, controlling behavior and alcohol consumption by the husbands was significantly associated with sexual violence. Women who had faced any one form of violence (physical or sexual) were at higher risk of facing the other form as well. 36% of women victims of IPV studied justified violence by husbands. Women who faced controlling behavior, experienced sexual violence, were poorly educated, or were married for more than 10 years were more likely to justify any form of IPV they faced. Alcohol consumption, controlling behavior, and justification of violence are important behavioral predictors for physical or sexual violence. This study concluded that there is a need for behavioral change communication strategies targeted at male partners and also the families to curb the menace of IPV (Joshi et al., 2020).
|
|
Jane's Story
My partner was very insecure about my past relationships and became jealous of anyone he thought might be ‘a threat’. At the beginning, it seemed almost charming – like he wanted to be number in my world… but over time it became more and more frightening. Whenever I went out, Max would want to know why, where I’d be and exactly who’d been there. If I came home later than I said, he’d accuse me of having an affair. If he’d been drinking, he’d call me a ‘f**king whore’ and other stuff. He would shout, swear and square up to me – it started happening multiple times a week. Next day he was always sorry and “felt so bad - he’d never do it again”. Over time he stopped me from talking with friends freely, he would throw and break things afterwards if I did. He’d drive the car at high speed with me in it, knowing I hated it and was petrified. I started to believe that Max’s behavior was my fault, like he said. My self-esteem was wrecked, and I spent most days crying. In the end it was my Family Doctor who helped me take the first step. She also wrote a letter for me; I was able to get legal aid and advice and was able to stand up to Max’s abuse and escape him.
|
|
Attachment Insecurity Impact on IPV
Significant indirect effects of attachment insecurity on IPV victimization through (a) socially prescribed (but not self-oriented) romantic perfectionism and (b) perceived couple conflict. Specifically, higher levels of attachment anxiety and attachment avoidance were indirectly associated with more IPV victimization (i.e., physical and psychological) through higher levels of socially prescribed romantic perfectionism and perceived couple conflict. This study highlights a viable mechanism underlying the link between romantic attachment insecurity and IPV victimization (Lafontaine, et al., 2021).
|
|
Greta's Story
At the start, I was so happy with Michael - he appeared very genuine and caring. Really charming. But then, our relationship began to change - he started to tell me that because of my dyspraxia I shouldn’t be in charge of finances. We met at the university, where I was a full time student but worked too, where I could. He didn’t - and because he was an international student he said he couldn’t work or access any grants or benefits. But he would frequently take money from me. And made me feel guilty if I refused to buy him stuff - he even asked for designer gifts. I trusted him, and he used this to get access to all my bank cards and details. It even turned out later he’d taken out a loan in my name. I started getting really suspicious when letters arrived about repayments that I could not afford. I felt worthless and so guilty for letting him into my life in the first place – like it was my fault! Finally, I confided in some friends: Jim and Connie, who suggested finishing the toxic relationship with Michael and reporting the bank fraud to the police. With their help and support, I was able to finish with Michael, get financial support, and rebuild my confidence and my life.
|
|
Victim's Subjective Suffering Influence Impact of IPV
In an operational psychodynamic diagnosis study, the severity of the violence was associated with the intensity of women’s subjective suffering. In the relational pattern, they stay in the relationship, leaving themselves vulnerable; perceive the partner as controlling, aggressive, offensive, and fear abandonment. As a defensive mechanism to relational discomfort and suffering victims anticipate the aggressor’s desire, resulting in submissive behavior. The main psychic conflict was the "need for care versus self-sufficiency" (78.6%). And medium was the predominant structure level, in which they presented insecure internal objects, presenting difficulties in emotional regulation and perceiving reality in a distorted way. Hence, they do not recognize their limitations and needs. It was found that 78.6% of the cases had some psychiatric disorder: MDD, PTSD (Both et al., 2020).
|
|
Mary's Story
Mary’s partner Vinny subjected her to years of abuse. He was very controlling and did not like her to leave the house. He did not let her have a mobile phone. Vinny had pulled a knife on her and threatened to kill her. He threatened to take their young child if she left him. A family member supported Mary to make a report to the Police about Vinny’s abuse. The Police temporarily removed their child on the advice of multi-agency practitioners. They were concerned that Mary was not acting protectively or able to protect their child from Vinny’s violence. Out of fear of his retribution for contacting the Police, Mary withdrew her Police statement. Vinny moved back in with her. Mary later separated from Vinny and proceeded with serious charges against him. These charges were before the courts at the time of her death. Mary’s next partner killed her. After Mary’s death, Vinny wanted custody of their child. Members of the maternal family also wanted custody. Vinny attended a short course on ‘anger management’. A plan was drafted….to transition the child back into Vinny’s care.
|
|
Reduced Quality of Life Due to IPV
An intimate relationship is an interpersonal relationship that involves physical or emotional intimacy. Those who are in such a relationship may experience violence from partners which may affect their day-to-day quality of life and thus cause a burden on the family. In a study of IPV victims The majority belonged to rural background and lower socioeconomic status. The study subjects reported poor and very poor scores in their overall quality of life and very dissatisfied and dissatisfied in their health domain. IPV also correlated with reduced quality of life, which was statistically significant. People that experience IPV have an overall reduced quality of life. Routine clinical assessment needs to be done to provide early interventions (Gopal et al., 2021).
|
|
Mark's Story
Mark, a 45-year-old man presented to his physician with a complaint of worsening depression. The patient had been taking antidepressant medications for many years, was receiving ongoing psychotherapy from a clinical social worker and attending Alcoholics Anonymous meetings. The patient complained of insomnia, loss of appetite and thoughts of guilt and suicide since his spouse had “kicked him out.” He was especially concerned because she has multiple sclerosis, relies on him for some physical assistance and, in his opinion, should not be left alone. Further discussion revealed that during an argument, he verbally threatened to harm her, then threw a large lamp at her (although he missed and did not actually hit her). She called the police, had him removed from the home and told him she would soon be filing for divorce.
|
|
Medical Implications of IPV
It is estimated that a majority of intimate partner violence (IPV) victims suffer from blunt force to the head, neck and the face area. Injuries to head and neck are among the major causes for traumatic brain injury (TBI). In a recent study findings suggested that health effects attributed to malnutrition, acquired thrombocytopenia, posttraumatic wound infection, local infection of wound, poisoning by cardiovascular drug, alcoholic cirrhosis, alcoholic fatty liver, and drug-induced cirrhosis which were highly significant at the joint presence of IPV and TBI. This study helped develop a better understanding of how IPV is related to negative health effects, it is potentially useful to determine the interactions and relationships between symptom categories. This study’s results can potentially improve the accuracy and confidence of existing clinical screening techniques on determining IPV-induced TBI diagnoses (Liu et al., 2020).
|
|
Sharon's Story
Legal aid contains collegiate stalker: “Sharon’s” physically violent ex-boyfriend continued to stalk her after they broke up. Her next problem arose when he started showing up on their college campus every time she left the library, computer lab or came out of her classroom. He repeatedly drove by her home and harassed her with constant telephone calls. Thinking that her only option was to drop out of school, Sharon sought help from LSC-funded West Tennessee Legal Services, which receives OVW LAV monies to help people like her. She and her legal aid attorney documented the stalking behavior, and together met with her college Dean to discuss the problem and proposed the distance her ex-boyfriend should maintain to keep Sharon safe. When her exboyfriend objected, Sharon’s attorney represented her in a court hearing, where the judge agreed with Sharon and issued a protective order with the specific distance she requested so she could continue her education.
|
|
Partner Stalking
Intimate partner stalking is a significant health and safety concern in the United States, yet research on this phenomenon remains minimal. A research study’s findings suggest that the victim’s marital status, suspect’s sex, suspect’s use of a firearm, geographic region of the homicide, and a documented history of abuse of victim by the suspect had significant relationships with homicide precipitated by intimate partner stalking. The associations between death by firearm and previously documented history of abuse with homicide precipitated by intimate partner stalking have substantial implications for the criminal justice system (Rai, et al., 2020).
|
Elaine's Story
Following a 911 call made to the police for help, ‘Elaine’ disclosed a 10-year history of domestic abuse but had never contacted police before because she was too embarrassed. She met her partner at the age of 17, and fell in love, but very quickly he became abusive. Elaine tells her story: “It started off slowly, and to begin with I thought he was being romantic and attentive. Always asking where I was going and who I was with, and he would say, ‘I just want to know you’re safe’. “But early one morning after a night out, I was awoken to the sound of my phone and he was screaming at me. Accusing me of being in bed with someone else. I tried to explain that I was in my friend’s house after not being able to get a taxi, but he just kept screaming. He told me I didn’t deserve to be treated this way. I thought he was confused, and he must have really thought I was with someone else. Somehow, his behavior got explained away, and I thought it was a blip. “A couple of weeks later though, we got home from a party we’d been to together. He started shouting at me again, telling me that I’d made a show of him, flirting with men at the party. That night he hit me, and then that became part of the norm. “Over time, I learned that socializing with my friends alone or with him just wasn’t worth the beating I would take afterwards. Even when he would go out though, he would phone me constantly just to check and see where I was and make sure I picked the phone up when I should. “Over time it became about more than going out though. He took my money so that I would have to ask permission to spend, because he said I was rubbish with finances. His constant checking up on me became so bad that in the end I just gave my job up. I was so lonely. And so ashamed. But I didn’t know how to escape. And after I became pregnant, it just seemed like that was how it was always going to be. “I finally left when, during another attack, he threw a bottle at me, and it narrowly missed our child. The next day I told my mom and sister what had been going on, and it was the most difficult thing to do ever. My sister helped me find the right support, and now I have my own home away from him. He doesn’t know where I am and I have a restraining order that keeps him away from me after that last assault. It was hard work, court is not easy at all, in fact it was probably harder than staying with him and putting up with it in some ways, but in my case, it was worth it. The life I have now is safe, my child is happy, and I look forward to things again rather than dread every life event. “If I could give anyone else advice, it would be to just tell someone. Don’t try and deal with it on your own, and don’t try and keep it a secret because you don’t need to.”
|
|
Cyber IPV
A study on cyber IPV, suggests that harmful electronic exchanges may have adverse consequences for young adults. The consequences include strain (i.e., depression and anger), substance use, and antisocial behavior among young adults. Males were also at higher risk for engaging in substance use and antisocial behavior across all models. The study suggests that harmful electronic exchanges may have adverse consequences for young adults. As such, services providers and educators addressing the issue of IPV should tailor prevention and intervention strategies in a way that is inclusive of cyber aggression and consider it a public health concern (Melander & Marganski, 2020)
|
|
Marcus's Story
Over a 15+ year period, Marcus had 20+ convictions for intimate partner violence offending against multiple female partners. More than three of his partners had obtained a protection order when they were attempting to separate from him. He breached each order multiple times. At the point of separation, Marcus had attempted to kill previous partners. In each instance his partner had been warned by a third party and police were able to apprehend him upon arrival at their homes. These events resulted in convictions, including threats to kill/do grievous bodily harm, breaches of restraining orders and possession of a weapon. Marcus was never imprisoned for his intimate partner violence offending. His sentence on his convictions for family violence offending near the end of his offending history was similar to the sentence he received at the beginning – supervision with Community Probation Service, and attendance at a non-violence program. He received warnings after breaching the restraining order against his last partner. Marcus killed his last partner when she was trying to separate from him. A third party called the police, but she died before they arrived.
|
|
Male Perpetrators of IPV
Intimate partner violence (IPV) takes several forms, such as physical and sexual violence, emotional and social abuse, threats and intimidation, and economic deprivation. For its prevalence and its harmful consequences, it has been defined as a salient public health issue. Studies about male perpetrators have often focused on individual risk factors and changing attitudes during IPV treatment. A current qualitative study aimed at extending past research on men attending IPV treatment, considering not only the individuals’ experience, but also the role of social and cultural dimensions, such as gender stereotypes and mass media. Three major themes emerged: the conception of violence and the influence of gender stereotypes; the process of change in the male perpetrators during treatment; and the social and cultural representation of male perpetrators. Findings highlight the necessity of taking into account the social and cultural contexts in which IPV occurs and provide robust support for the adoption of an ecological approach to IPV (Rollero, 2020).
|
Rick's Story
I was 23 at the time I met Anthony through work when I was 22. The relationship seemed okay in the beginning, but in hindsight, there were warning signs of what was to come. They were little things at first: coming over unannounced; showing up unexpectedly when I was out with my friends; phone calls that seemed to be a little too frequent. I made the mistake of interpreting these early signs as strong romantic interest. Before long he had moved in with me and his behavior had become obsessive and controlling. Anthony was really threatened by my friends and my social life. He hated that other guys would look at me, or that I’d slept with other guys around our neighborhood, even that I had quite a lot of friends who he felt “competed” with him. Tiny things that had not even occurred to me as being possibly offensive would cause enormous rage. The more I was attacked, the more and more I withdrew. It was a self-defense mechanism – I figured if I could stay away from anything that might cause him to get upset then that would keep him calm. That didn’t work of course – he simply found new things to be insecure about. I realize now the whole strategy was to keep me feeling perpetually blamed, inadequate and not doing enough to keep the relationship together. I isolated myself from my friends, my family and from everything that I used to enjoy doing. To get me away from my previous life, friends and sex partners we moved to a different city where I knew no one except him. I was by nature a very happy, outgoing person, but I quickly became cautious and scared all the time. My fear escalated when the physical violence began. The first time was because he had seen me talking to someone, I’d had a fling with in the past and he punched me in the face because of it. From that time on, even though the physical violence was occasional, the fear of it happening pervaded my life and he would threaten me with it often. Punching, pushing, restricting my physical movements (like blocking doors if I was trying to leave a heated situation), destroying or giving away my property and refusing to take care of me if I was sick were punishments that would be meted out when simply threatening me or humiliating me in public wasn’t enough. Anthony was from a racial minority. One of the biggest headfucks was being told that the violence was part of his “culture” and the fact that I had a problem with it meant that I was racist. The problem according to him was not the violence – it was the fact that my racism meant I couldn’t accept who he was. It was me not him, that had to change. I now understand that violence is not culture – there is no ethnic group on the planet that celebrates partner abuse as a cultural identity. Apart from my massive social withdrawal, the effect on my sexuality was really destructive. I became ashamed about being gay, about being sexually attractive and about having sexual desires. It was like going back in the closet. Money was another big problem. Successive rent periods came where Anthony would spend all of his pay on gambling and alcohol within 48 hours of receiving it, leaving me to pay all the rent and then provide food for us for a fortnight – impossible and it meant instant poverty. As a “solution”, Anthony put me in control of his finances, but it was only a license for him to be as irresponsible as he liked and simply demand more money whenever he wanted it. Of course, refusing because the rent needed to be paid for example, was a dangerous move. On top of all of this, he would also frequently get me to do his work for him. It wasn’t uncommon for me to be producing his reports until all hours of the morning while he watched TV. I had given up on my life ever being enjoyable again. My whole sense of individual identity was gone, and I felt as though I barely existed. A lesbian friend from the previous city I lived in sent me a book about SM sub-cultures (one of her favorite things) that contained a chapter on the difference between an SM relationship and domestic violence. There was a checklist of questions to ask yourself to determine whether you were in an abusive relationship and when I found I was answering yes to almost everything, a crack appeared in the brainwashing and manipulation that had filled my head. I suddenly realized that I had to accept that I was in a domestic violence relationship. I took the grand leap of confiding in someone I worked with about my situation and one afternoon, after Anthony threatened to “break both my legs” when I got home that night, this colleague generously lent me his spare room for a week while I “disappeared” from my home. During that week I found a new place to live and, with a Gay and Lesbian Police Liaison Officer, I went to pick up my belongings and left. A new phase of harassment and stalking that included a wide range of manipulations and threats (ranging from “Come back - I’ve changed!” to “If you have sex with another man I’ll kill you and him”) followed.
|
|
LGBT IPV
Intimate Partner Violence (IPV) is a prevalent but under recognized issue among sexual minorities broadly, but especially among Black Gay and Bisexual Men (BGBM). Over the last several years, acts of IPV among BGBM made national news, drawing attention to the unique ways that IPV plays out within this particular population. Yet, little research has examined the intersections between race and sexuality among BGBM, the lack of culturally responsive IPV services, their support needs, or the barriers that BGBM face when seeking IPV related services. When examined closely, the feld of IPV has traditionally focused on cisgender heterosexual white women as victims and cisgender white men as perpetrators, which has historically impacted the availability and quality of IPV services for other populations. This narrative critique of the IPV movement calls for an intersectional social justice and health equity approach to address the unique and intersectional needs of BGBM who experience IPV. By centering the intersectional needs of BGBM and the role that racism, homophobia, and heteronormativeness has played in shaping IPV-related services, this article challenges the IPV feld to advance a social justice orientation in order to address the unmet needs of BGBM who experience IPV (Brooks et al., 2021).
Sexual minority (SM) youth are at high risk for intimate partner violence (IPV) and suicidal ideation/attempts compared to their heterosexual peers. A study examined whether SM identity enhanced the relationship between experiences of IPV and suicidal ideation/attempts. Each SM identity and both physical and sexual IPV were significantly associated with suicidal ideation and suicide attempts. The interaction between bisexual identity and physical IPV was significant for suicidal ideation; as physical IPV experiences increased, the difference between bisexual identity and heterosexual youth was non-significant. These findings suggest exploring trauma and suicidal ideation by aggregate groups and increasing support for SM youth in schools and communities (Nydegger, et al., 2020).
|
|
Kim's Story
She was my brother’s friend. Someone who was mysterious and extremely funny and entertaining. Small in stature, chocolate colored with a beautiful androgynous face and a mischievous smile. My brother had told me about Vivian as she had the same name as another of his friends and he differentiated between them by color. I was young and about to leave home for the second time and planned to live with my brother until I was sure-footed once again in the big bad world. John and I decorated a room in readiness, and I felt free once again. My brother, a gay man, had many friends and I got to know most of them. They were kind and generous to me and most helped me on my way as a young lesbian. Viv had immediately intrigued me and started to visit my brother regularly. It was a while before my attraction to her was noticed then she would smile every time she saw me. She would come round and make us laugh and we would smoke a few joints and just not be able to stop. My brother noticed my attraction and warned me off getting involved with her but could never tell me why. What did he know about lesbians? We became lovers soon after I moved in and she fell in love with me and opened her tortured heart. Viv had a lot of things just not going her way. She was on the dole, her heart had been broken by a very nasty piece of work and her mother, brother and sister were poor and lived in the rooms above her granny flat. She came from a mixed-race family and her father had left her when she was six. She wanted to be tall and become a blues musician - everyone had got her wrong. I wanted to rescue her, give her my heart and everything. I had to heal those wounds and show her a love that was real and let her know how talented she really was. However, after six months together I knew something wasn’t right. I felt I had got myself into something that perhaps wasn’t very good for me, but I wasn’t going to let my friends and family know I had made a mistake. This was a relationship that was going to work. Viv smoked a lot of drugs and took a lot of speed. She needed dope to wake up, speed to party and get herself through the day and dope to bring her down and help her sleep. She never wanted to take drugs by herself and it became a priority on our shopping list. I say this because drugs would deepen the moods and fuel the sudden changes and verbal attacks. She wasn’t physically violent at that stage but was capable of shooting me down in words and making me feel humiliated and scared. I left my brother’s after a big row that was instigated and fueled by Viv. She managed to drive a huge wedge between my brother and I. I didn’t speak to my brother until the relationship with Viv came to an end three years later. I moved into her granny flat underneath her family in a big, run down, Edwardian house. Two years had gone by and I was starting to look ill. I had lost an enormous amount of weight through nerves and drugs and had isolated most of my friends. We would only go and see friends that she trusted. She said I was wasting my time with members of my family and friends as they didn’t understand me and didn’t understand us. Sex between us had dwindled and I began to feel nauseous whenever she would touch me. The good times together were getting few and far between. She controlled my days, my social calendar, the clothes that I wore and the people I would speak to. She kept me from going to see my family by starting a big row just before I would leave. My sanctuary was my work. How I managed to work and survive this relationship I don’t really know but eventually the phone calls at work started. After three years, I was extremely unhappy with no one to talk to. Something was happening to me that nobody could know about. I was ashamed and afraid of what people would think. When she had taken speed during the day, I knew we would be arguing all night. She wouldn’t let me sleep until I had come round to her point of view. She would argue points again and again until I would fall asleep staring at her, which would start her off once again. I thought if we moved into a place, we could call our own everything would be better. I borrowed money, got a mortgage, and told her that she now had a home of her own to share with me and that I loved her. From now on things were going to get better. They never did. Eventually when the calls at work became embarrassing and I would have to leave work to go home and row with her, physical fights started to happen. She hit me and I hit her back and I started to feel sick but couldn’t pull away from the relationship. All our friends knew by now and would avoid us because Viv would like to humiliate me in front of them. One good dear friend who is now dead, said that one day I would find the strength and that he and his boyfriend would support my decision. He was one of Viv’s closest friends and I started to think about things and talk to people and decided enough was enough. The end was very messy. I had to be sneaky and think carefully about how I would pull this off. No dramatics - I was exhausted. I had to distract her from what was going to happen, and I hated myself for it but I wanted peace. Eventually it would come, but at a price. That relationship, while enriched with valuable lessons, left me sick and untrusting of anybody for a very long time but eventually I fell in love again. We lived in a small town but whenever Viv and I would meet she looked right through me as if I didn’t exist. She had been betrayed. Nobody could understand why we weren’t friends. Healing for me has been talking about it and here I am eighteen years later still talking about it.
For more on stories of Intimate Partner Violence in the LGBT Community go to:
Tales from Another Closset - Personal Stories of Domestic Violence in Same-sex Relationships
|
|
IPV of Young Men
Among young US men, 9 in 10 support IPV identification by health care clinicians, nearly 1 in 5 report using IPV, but only about 1 in 10 report health care clinicians asking about IPV. These represent missed opportunities for health care IPV identification. Beliefs and experiences regarding health care IPV identification vary by race, education, and men’s IPV perpetration and victimization. These disparities can inform tailored health care identification approaches. Of men who participated this study, 19% reported perpetration and 27% reported victimization in relationship with current or previous spouse/partner, 90% believed health care clinicians should ask about perpetration, 92% believed health care clinicians should ask about victimization, but only 11% had been asked about perpetration and 13% about victimization. Beliefs regarding IPV were associated with African American non-Hispanic race, IPV perpetration, and IPV victimization. Experiences being asked about IPV were associated with educational attainment and IPV perpetration (Walsh, et al., 2020)
Transgender IPV
Transgender individuals experience a dramatically higher prevalence of IPV victimization compared with cisgender individuals, regardless of sex assigned at birth. IPV prevalence estimates are comparably high for assigned-male-sex-at-birth and assigned-female-sex at-birth transgender individuals, and for binary and nonbinary transgender individuals, though more research is needed. Evidence-based interventions are urgently needed to prevent and address IPV in this high-risk population with unique needs. Lack of legal protections against discrimination in employment, housing, and social services likely foster vulnerability to IPV. Transgender individuals should be explicitly included in US Preventive Services Task Force recommendations promoting IPV screening in primary care settings. Interventions at the policy level as well as the interpersonal and individual level are urgently needed to address epidemic levels of IPV in this marginalized, high-risk population (Peitzmeier, et al., 2020).
|
|
Marianna's Story
I got married at the age of 18 and believed our lives would be perfect. When my ex-partner got his way, he was wonderful. When he didn’t, he would blame me whether it was my fault or not. If I got upset or challenged him, he would say I was weak and didn’t know what I was doing. I started to find food I thought I had bought disappearing and he would say I was stupid. I would arrive at a pre-booked appointment at the hairdressers and find it was cancelled. I missed school evenings because the dates I was told were incorrect. I thought I was losing my memory or my sanity. He used to try to exclude me when we attended gatherings, whispering to tell me to leave because I wasn’t welcome. If I got upset, he would make it look like I had mental health issues and I was being oversensitive. He eventually stopped me from seeing my friends and family, telling me that I only needed him in my life, and they all thought I was stupid. I eventually became too afraid to do anything or make any decisions because I knew they’d be wrong, and I would be threatened. As a result of the constant insults from my ex-partner, I lost 30 pound and was referred to a counselor. With the support of my counselor and family lawyer, I have now got a Restraining Order against my ex-partner and I have started divorce proceedings.
|
|
Treatment of IVP Effectiveness
A review of the effectiveness of interventions for IPV offenders included motivational strategies to reduce physical and psychological IPV, treatment dropout, official recidivism to IPV offending, and to increase intervention attendance dose. IPV interventions that incorporated motivational strategies were significantly more effective in increasing the intervention dose and reducing dropout than interventions without motivational strategies. IPV offenders receiving interventions with motivational strategies were 1.73 times less likely to intervention dropout compared to those in interventions without such strategies. For physical and psychological IPV and official recidivism (e.g., rearrests, police record), evidence favored interventions with motivational strategies, although not significantly. These findings have important practical implications, especially considering the high dropout rates in IPV offender programs and the link between dropout and higher rates of recidivism (Santirso et al., 2020).
Intimate partner violence (IPV) is a key public health issue, with a myriad of physical, sexual and emotional consequences for the survivors of violence. Social support has been found to be an important factor in mitigating and moderating the consequences of IPV and improving health outcomes. There is good evidence of the effect of IPV interventions focused on improving access to social support through the use of advocates with strong linkages with community based structures and networks, on better mental health outcomes of survivors (Ogbe et al., 2020).
|
|
Sarah' Story
Sarah has been receiving messages from her ex-partner telling her that when his Restraining Order expires early next year she will need to “deal with him directly”. Sarah understands that he means he will be coming to her home address again. Sarah ended the relationship with her ex-partner five years ago and he has been issued with numerous restraining orders since this date which he has breached every time. Sarah contacted the police and told them that her ex-partner had not breached the current order, but she wanted the matter logged anyway because she was fearful, however, during a joint visit between a member of the Community’s Domestic Abuse Team and Community’s Police there were concerns from professionals that the order had in fact been breached. Sarah has received guidance and support from the Police and Domestic Abuse Team, giving her the confidence to work with all the services available to her in order to deal with the text messages she has been receiving.
Sarah says: “I know no-one can stop him – only he can stop what he’s doing. But knowing that people understand what’s happening in the same way as I do makes all the difference as to how you’re able to cope with the situation. I know I can deal with this.”
|
|
Types of social support interventions for IPV survivors
Survivor-focused social support interventions
Advocacy/Case management interventions
Advocacy/Case management interventions with a psychotherapy component
Community-focused/network social support intervention
Community-focused/network interventions with a psychotherapy component
Findings: Advocacy/case management interventions that had strong linkages with communities, and were community focused seemed to have significant effects on mental health outcomes and access to resources for IPV survivors (Ogbe et al., 2020)
|
|
Amy's Story
Four years after Amy first fell in love with her husband, he killed her while her children waited for her outside their home. “Someone call 911. I just shot Amy,” said Vincent, as he stumbled out the door, but she was already dead. She was 33. Their love affair started in 1997 in State College, Pennsylvania, where she worked in a home store; he drove the armored truck that picked up money from the shop. And shortly after they met, they had their first son. Before they had a child, Vincent started driving her to work and picking her up every day. He called the store incessantly. He checked her schedule to make sure she wasn’t working alone with men. Then there were the bruises that came from “softballs” and “falling boxes.” But there was no way to connect the dots at the time. Amy’s co-workers noticed strange behavior, going so far as to draft a fake schedule to throw Vincent off track. Amy’s parents drove her to the police station to get a protection order. But the incidents seemed disjointed, and no one realized that it would lead to murder.
The danger signs in Amy’s abusive relationship—and more important, the number of times that police or other services could have intervened. Something that seems so obvious in hindsight wasn’t when Amy was in the depths of it. That seems to be the question on most people’s minds about domestic violence. Why didn’t she leave? The question irks domestic-abuse advocates to no end. “‘Why doesn’t she leave?’ needs to be ‘why does he beat her?’” “You can’t put the burden on the victim.” At times, it seemed that Amy herself was the only person who could pull it all together and make a change. But between their deeply intertwined lives and the sheer terror, she was in no place to take on that burden, even if it was hers to begin with. And the terror, as it turns out, was founded. Vincent killed her when she went home to gather her things for the final time.
|
|
Impact of MBSR & CBGT Intervention
Violence in close relationships is a global public health problem and there is a need to implement therapeutic programs designed to help individuals who voluntarily seek help to reduce recurrent intimate partner violence. The effectiveness of such interventions in this population remains inconclusive. The aim of a current study was to compare the effectiveness of cognitive-behavioral group therapy (CBGT) vs mindfulness-based stress reduction (MBSR) group therapy in reducing violent behavior among individuals who are violent in intimate partnerships and who voluntarily seek help. Results of their study provided support for the efficacy of both the cognitive-behavioral group therapy and the mindfulness-based stress reduction group therapy in reducing intimate partner violent behavior in men voluntarily seeking treatment (Nesset, et al., 2020).
|
|
Nazia's Story
Her Legal Aid lawyer helped prevent abuse and treat trauma and contained a collegiate stalker. “Nazia,” a 37-year-old immigrant from Guyana, fled with her two young children from the physical and emotional abuse of her husband. With the assistance of Queens Legal Services (QLS), a recipient of HHS FYSB funding, she successfully obtained an Order of Protection and full custody of her children. However, shortly thereafter, Nazia’s abuser retaliated by filing for a modification of custody, citing frivolous allegations of inappropriate parenting. Her legal aid lawyer continued to represent her and also referred Nazia to a QLS social worker, who provided counseling to her and her children throughout the process. Again, thanks to her legal aid lawyer, after two years of litigation, Nazia settled the case and retained sole legal custody of her children.
|
|
References
Avanigadda, D.B. & Kulasekaren, R.A. (2021). Associations between intimate partner violence and pregnancy complication: A cross-sectional study in India. Journal of Family and Community Medicine,28(1), 17-27. DOI: 10.4103/jfcm.JFCM_256_20
Basile, K.C., Hertz, M.F., Back, S.E. (2007). Intimate partner violence and sexual violence victimization assessment instruments for use in healthcare settings: Version 1. Atlanta (GA): Centers for Disease Control and Prevention, National Center for Injury Prevention and Control
Both, L.M., Favaretto, T.C., Freitas, L.H.M., Benetti, Sd.C, & Crempien, C. (2020) Intimate partner violence against women: Operationalized Psychodynamic Diagnosis (OPD-2). PLoS ONE 15(10): e0239708. https://doi.org/10.1371/journal. pone.0239708
Brooks, D., Wirtz, A.L., Celantano, D., Beyer, C., Hailey-Fair, K. & Arrington-Sanders, R. (2021). Gaps in science and evidence-based interventions to respond to intimate partner violence among black gay and bisexual men in the U.S.: A call for intersectional social justice approach. Sexuality & Culture, 25, 3060317. Doi.org/10.1007/s12119-020-09769-7
Chan, C.S., Sarvet, A.L., Basu, A., Koenen, K. & Keyes, K.M. (2021). Associations of intimate partner violence and financial adversity with familial homelessness in pregnant and postpartum women: A 7-year prospective study of the ALSPAC cohort. PLoS ONE 16(1), e0245507. https://doi. org/10.1371/journal.pone.0245507
Gopel, N.R., Kumar, S.S. & Bhat, K.S. (2021). Association between intimate partner violence with quality of life. Journal of Clinical and Diagnostic Research, 15(1), VC01-VC04. DOI: 10.7860/JCDR/2021/46088.14426
Hellmuth, J.C. & Leonard, K.E. (2013). Methods of assessing and addressing participant protection concerns in intimate partner violence research. Partner Abuse, 4(4), 482-493. doi:10.1891/1946-6560.4.4.482.
Joshi, R.K., Arora, M. & Mukherjee, R. (2020). Do women justify the violence they face? Intimate partner violence among married women. Medical Journal of Dr. D.Y. Patil Vidyapeeth, 13:113-9. DOI: 10.4103/mjdrdypu.mjdrdypu_255_18
Klostermann, K., Mignone, T., Kelley, M. L., Musson, S., & Bohall, G. (2012). Intimate partner violence in the military: Treatment considerations. Aggression and Violent Behavior, 17(1), 53-58.
Lafontaine, M.F., Azzi, S., Bell-Lee, B., Dixon-Luinenburg, T., Guerin-Marion, C. & Bureau, J.F. (2021). Romantic perfectionism and perceived conflict mediate the link between insecure romantic attachment and intimate partner violence in undergraduate students. Journal of Family Violence, 36, 195-208.
Leuenberger, L., Lehman, E. & McCall-Hosenfeld, J. (2021). Perceptions of firearms in a cohort of women exposed to intimate partner violence (IPV) in central Pennsylvania. BMC Women’s Health, 21(20) https://doi.org/10.1186/s12905-020-01134-y
Liu, L.Y., Bush, W.S., Koyuturk, M. & Karakurt, G. (2020). Interplay between traumatic brain injury and intimate partner violence: Data driven analysis utilizing electronic health records. BMC Women’s Health, 20:269.
https://doi.org/10.1186/s12905-020-01104-4
Lynengar, R. & Sabik, L. (2009). The dangerous shortage of domestic violence services. Health Affairs, 28, 6; ProQuest One Academic W1052
Lyengar, R., Bondade, S. & Raj, R. (2020). A cross sectional hospital-based study of intimate partner violence and psychiatric comorbidity in pregnancy. Archives of Psychiatry and Psychotherapy, 4, 12-21. Doi: 10.12740/APP/120441
Maluneh, M.D., Alernu, Y.W. & Meazaw, M.W.(2021). Geographic variation and determinants of help seeking behaviour among married women subjected to intimate partner violence: evidence from national population survey. International Journal for Equity in Health, 20, 13. DOI https://doi.org/10.1186/s12939-020-01355-5
Melander, L. A., & Marganski, A. J. (2020). Cyber and in-person intimate partner violence victimization: Examining maladaptive psychosocial and behavioral correlates. Cyberpsychology: Journal of Psychosocial Research on Cyberspace, 14(1), 1. https://doi.org/10.5817/CP2020-1-1
Nesset, M.B., Lara-Cabrera, M.L., Bjorngaard, J.H., Whittington, R. & Palmstierna, T. (2020). Cognitive behavioral group therapy versus mindfulness-based stress reduction group therapy for intimate partner violence: A randomized control trial. BMC Psychiatry, 20:178 https://doi.org/10.1186/s12888-020-02582-4
Nydegger,L,A,, Blanco, L., Marti, C.N., Kreitzberg, D.& Quinn, K. (2020), Evaluation of sexual minority identity as a moderator of the association between intimate partner violence and suicidal ideation and attempts among a national sample of youth. PLoS ONE 15(8): e0236880. https://doi.org/ 10.1371/journal.pone.0236880
Ogbe, E., Harmon, S., Van den Bergh, R. & Degomme, O. (2020). A systematic review of intimate partner violence interventions focused on improving social support and/mental health outcomes of survivors. PLoS ONE 15(6), e0235177. https://doi.org/10.1371/journal. pone.0235177
Peitzmeir, S.M., Malik, M., Kattari, S.K., Marrow, E., Stephenson, R., Agenor, M. & Reimer, S.L. (2020). Intimate partner violence in transgender populations: Systematic review and meta-analysis of prevalence and correlates. American Journal of Public Health, 110, e1-e14. doi:10.2105/AJPH.2020. 305774
Rai, A., Villarreal-Otalora, T., Blackburn, J. & Choi, J. (2020). Correlates of intimate partner stalking precipitated homicides in the United States. Journal of Family Violence, 35, 705–716. https://doi.org/10.1007/s10896-020-00137-5
Rollero, C. (2020). The social dimensions of intimate partner violence: A qualitative study of male perpetrators. Sexuality & Culture, 24, 749-763. https://doi.org/10.1007/s12119-019-09661-z
Rubin, A., Weiss, E.L. & Coll, J.E. (2012).Handbook of military social work. John Wiley & Sons: New Jersey.
Santirso, F.A., Gilchrist, G., Lila, M. & Gracia, E. (2020). Motivational strategies in interventions for intimate partner violence offenders: A systemic review and meta-analysis of random controlled trials. Psychosocial Intervention, 29(3), 175-190.
Sprague, S., Madden, K., Simunovic, N., Godin, K., Pham, N.K., Bhandari, M. & Gosslings, J.C. (2012) Barriers to screening for intimate partner violence. Women & Health, 52(6):587-605. doi: 10.1080/03630242.2012.690840.
Taft, C. T., Macdonald, A., Monson, C. M., Walling, S. M., Resick, P. A., & Murphy, C. M. (2013). “Strength at home” group intervention for military populations engaging in intimate partner violence: Pilot findings. Journal of Family Violence, 28(3), 225-231.
Tasso, A., Whitmarsh, L., & Ordway, A. (2016). Intimate partner violence within military families: Intervention guidelines for relational aggressors. The Family Journal. Advance online publication. doi:10.1177/10664807166286221066480716628 622
Tolley, E.E., Zissette, S., Martinez, A,, Palanee-Phillips, T., Mathebula, F., Tenza, S., et al. (2020) Development and initial validation of a simple tool to screen for partner support or opposition to HIV prevention product use. PLoS ONE 15(12): e0242881. https://doi.org/10.1371/journal.pone.0242881
Tower, L.E. (2006), Barriers in screening women for domestic violence: A survey of social workers, family practitioners, and obstetrician– gynecologists. Journal of Family Violence, 21(4):245-257.
Viejo, C., Linde-Valenzuela, G. & Ortega-Ruiz, R. (2018). Adult Partner Violence and Previous Violence Experiences: Retrospective Study with Women Victims of Gender-based Violence. International Journal of Psychology & Psychological Therapy, 18, 179-192.
Walsh, T., Seabrook, R.C., Tolman, R.M., Lee, S.J. & Singh, V. (2020). Prevalence of intimate partner violence and beliefs about partner violence screening among young men. Annals of Family Medicine, 19(4), 303-308. DOI: https://doi.org/10.1370/afm.2536
Woods, A.B., Page, G.C., O’Campo, P., Pugh, L.C., Ford, D. & Campbell, J.C. (2005). The mediation effect of posttraumatic stress disorder symptoms on the relationship of intimate partner violence and IFN-y levels. American Journal of Community Psychology, 36(1/2), 159-179. DOI: 10.1007/s10464-005-6240-7.
Zero, O. & Geary, M. (2020). COVID-19 and intimate partner violence: A call to action. Rhode Island Medical Journal
|
|
|